A Cross-Sectional Study on the Distribution of Hemoglobin Levels Among Pregnant Women in Quetta, Balochistan
-
Halima Khalid
Department of Biotechnology, Faculty of Life Sciences and Informatics, Balochistan University of Information Technology, Engineering and Management Sciences, Quetta, Pakistan
Sobia Faisal MalikDepartment of Environmental Science, Faculty of Life Sciences and Informatics, Balochistan University of Information Technology, Engineering and Management Sciences, Quetta, Pakistan
Fatima IqbalMultan Cancer Clinic, Nishtar Chowk, Nishtar Road, Multan, Pakistan
Shakeela Daud

Department of Biotechnology, Faculty of Life Sciences and Informatics, Balochistan University of Information Technology, Engineering and Management Sciences, Quetta, Pakistan
| Received 12 Nov, 2025 |
Accepted 20 May, 2026 |
Published 30 Sep, 2026 |
Background and Objective: Iron deficiency anemia (IDA) is the most common nutritional disorder among pregnant women worldwide, posing a serious threat to both maternal and fetal health. The objective of this study was to determine the prevalence and severity of iron deficiency anemia in pregnant women in Quetta District, Balochistan, and to compare hematological parameters between trimesters. Materials and Methods: A survey, laboratory tests, and a cross-sectional study were conducted at Civil Hospital Quetta, involving 75 randomly sampled pregnant women. Blood was analyzed using a Complete Blood Count (CBC) to measure key hematological parameters such as Hemoglobin (Hb), Mean Corpuscular Volume (MCV), Mean Corpuscular Hemoglobin (MCH), Mean Corpuscular Hemoglobin Concentration (MCHC), and Hematocrit (HCT). Data were analyzed using Microsoft Excel to compute frequencies, percentages, and mean±standard deviation, with statistical significance considered at p<0.05. Results: 80% of participants had hemoglobin levels between 10-11 g/dL, indicating a high prevalence of anemia. All hematological parameters were below the reference range, supporting a diagnosis of microcytic hypochromic anemia typical of iron deficiency. The prevalence of anemia was highest in the second trimester, coinciding with increased physiological iron requirements. Conclusion: These findings highlight iron deficiency anemia as a significant public health issue among pregnant women in Quetta, driven by poor dietary habits, low adherence to supplementation, and socioeconomic factors. There is an urgent need to improve nutritional education, make routine antenatal screening mandatory, and increase access to iron and folic acid supplements to reduce maternal anemia and improve pregnancy outcomes in resource-limited settings.
| Copyright © 2026 Khalid et al. This is an open-access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. |
INTRODUCTION
Iron deficiency anemia (IDA) remains a major global health problem, particularly affecting women of reproductive age. According to the World Health Organization1, anemia during pregnancy is defined as hemoglobin levels below 11 g/dL in the first and third trimesters, and below 10.5 g/dL in the second trimester. Approximately 36.5% of pregnant women worldwide suffer from anemia, with the burden disproportionately higher in low- and middle-income countries2.
Iron is an essential micronutrient required for the synthesis of hemoglobin and oxygen transport. During pregnancy, blood volume increases by nearly 50%, increasing iron requirements to support fetal growth and placental development3. In Pakistan, iron deficiency anemia is particularly common in underserved areas like Quetta, where limited healthcare access, poverty, and poor nutritional awareness contribute to its prevalence4.
Preterm birth, low birth weight, intrauterine growth restriction, and increased maternal morbidity are just a few of the negative outcomes linked to IDA during pregnancy5. This study focuses on analyzing the hemoglobin distribution and hematological profiles of pregnant women in Quetta District to understand the extent and biological implications of IDA.
MATERIALS AND METHODS
This study used simple random sampling. The sampling frame included all pregnant women who attended the antenatal Outpatient Department (OPD) at Civil Hospital Quetta from April to June 2025. A list of eligible women was obtained from hospital records. Each woman was assigned a unique number, and 75 participants were randomly selected.
Study population: The study population consisted of pregnant women visiting the antenatal clinic at Civil Hospital Quetta during the study period. Women were enrolled regardless of their trimester, ensuring a diverse sample representing different stages of pregnancy.
Sample size and sampling technique: A total of 75 pregnant women were selected through random sampling. This approach was used to reduce selection bias and give each eligible woman attending the clinic an equal opportunity to participate.
Inclusion and exclusion criteria: Pregnant women of any age and trimester who attended antenatal care at Civil Hospital Quetta during the study period and were willing to participate with informed written consent. Women with pre-existing chronic illnesses or who were on medication that could affect hematological parameters were excluded. Participants who declined to take part were also excluded.
Ethical considerations: The study was approved by the Institutional Ethical Review Committee of the Department of Biotechnology, BUITEMS, Quetta, Pakistan. Written informed consent was obtained from all participants before data collection.
Data collection procedure: Data was collected using a structured questionnaire and laboratory analysis. After obtaining informed consent, participants were interviewed to obtain demographic and obstetric information, including age, gestational trimester, dietary habits, and use of iron supplements.
Blood sample collection: Venous blood (2-3 mL) was drawn from each participant and collected in EDTA tubes. Hematological parameters, including Hemoglobin (Hb), MCV, MCH, MCHC, and HCT, were measured using an automated hematology analyzer (Huma Count 80 TS). All data were recorded and coded for analysis.
Laboratory analysis: Samples were analyzed with a Huma Count 80 TS hematology analyzer. The CBC tests provided values for Hb, MCV, MCH, MCHC, and HCT. Standard reference ranges were used for comparison6,7.
Data analysis: Blood tubes placed on the rollers rotate horizontally and gently roll back and forth. This prevents the cells from settling at the bottom. Since the tubes contain anticoagulant (EDTA), rolling helps keep the blood evenly mixed. To avoid clot formation and ensure that red cells, white cells, and platelets are evenly suspended. The dial (on the front) lets you set the speed (up to 70 RPM) for 3-5 minutes.
Before running the sample on a hematology analyzer, Human Count 80 TS. A small amount of blood is aspirated by the analyzer. The blood is diluted with a special diluent to separate cells for counting. The sample is divided into different chambers for RBC, WBC, and platelet counts. The concentration is measured using spectrophotometry. The analyzer’s software calculates RBC, WBC, Platelet count, Hemoglobin, Hematocrit, MCV, MCH, and MCHC. Results are shown on the screen.
Data was entered and analyzed using Microsoft Excel. Descriptive statistics, including frequencies and percentages, were calculated for hematological parameters such as hemoglobin (Hb), MCV, MCH, MCHC, and HCT. Results were presented in tables and figures for clear interpretation. Where applicable, comparisons between trimesters were assessed, and a significance level of p<0.05 was considered statistically significant.
RESULTS
A total of 75 pregnant women were included in the study. Most participants had hemoglobin levels between 10-11 g/dL, indicating mild anemia based on WHO criteria. The mean (±SD) value of Hemoglobin (Hb) was 10.5±0.6 g/dL, indicating reduced oxygen-carrying capacity. Mean corpuscular volume (MCV; 75-80 fL), Mean Corpuscular Hemoglobin (MCH), and Mean Corpuscular Hemoglobin Concentration (MCHC) were all below normal reference ranges, confirming microcytic hypochromic anemia. Hematocrit (HCT) values also averaged 27.2-29.2%, supporting the diagnosis of anemia. Second-trimester women demonstrated the highest frequency of anemia, followed by the third and first trimesters.
Table 1 outlines the criteria for anemia based on Red Blood Cell (RBC) parameters. Each parameter helps determine whether a person, especially a pregnant woman, is anemic, and the type of anemia.
| Table 1: | Diagnostic criteria for anemia based on hematological parameters (Hb, MCV, MCH, MCHC, and HCT) used to classify iron deficiency anemia among pregnant women | |||
| Parametets | Anemic range |
| Hemoglobin | 10-11 g/dL |
| MCV | <80 fL |
| MCHC | <320-360 g/L |
| MCH | <29 pg |
| HCT | <33% |
|
|
|
|
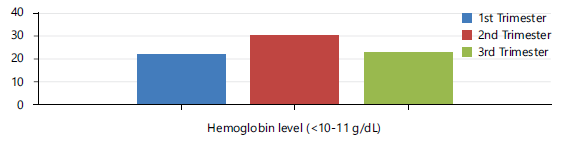
Hemoglobin levels: The highest frequency of low hemoglobin values was observed in the second trimester (around 30 patients), followed by the third trimester (about 22 patients) and first trimester (about 21 patients). This indicates that anemia prevalence peaks in the second trimester, consistent with increased iron requirements due to fetal growth and increased maternal blood volume. The second trimester is the most vulnerable to iron deficiency anemia. Hemoglobin levels rarely exceed 11 g/dL, suggesting mild anemia among the studied population according to the WHO criteria for pregnancy in Fig. 1.
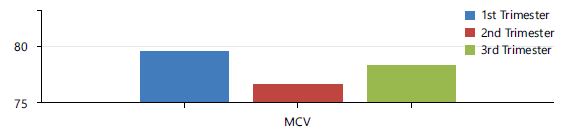
Mean Corpuscular Volume (MCV): The MCV values (in femtoliters, fL) range between 75-80 fL for all trimesters. The first trimester recorded the highest MCV (~79.5 fL), followed by the third trimester (~78 fL), and the second trimester showed the lowest (~76 fL). Since normal MCV is 80–100 fL, all values fall below the normal range, indicating microcytic anemia, a characteristic feature of iron deficiency anemia in Fig. 2.
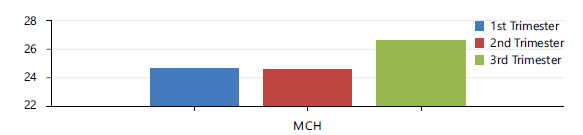
Mean Corpuscular Hemoglobin (MCH): Mean corpuscular hemoglobin (MCH) values across trimesters are presented in Fig. 3. The results indicate that MCH values remain below the normal reference range in all trimesters, with slightly higher values observed in the third trimester. This trend suggests persistent hypochromic anemia among the study population, with minimal improvement as pregnancy continues.
|
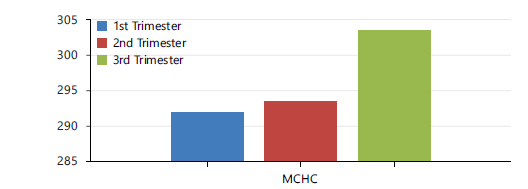
The MCHC values (g/L) show a gradual increase across trimesters: First trimester: ~292 g/L, Second trimester: ~294 g/L, Third trimester: ~303 g/L. Although still slightly below the normal reference (320–360 g/L) in Fig. 4, an upward trend indicates some recovery or adaptation in later pregnancy stages. An initial low MCHC reflects hypochromia in early pregnancy.
The MCHC increased slightly across trimesters (292-303 g/L) but remained below normal (320-360 g/L), suggesting persistent anemia.
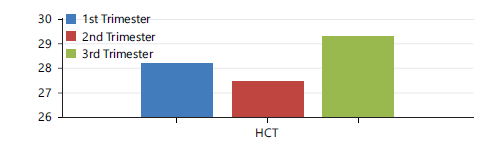
Hematocrit (HCT): In Fig. 5 HCT ranged from 27.2-29.2%, below the standard 33-39%, confirming anemia severity, especially in the second trimester.
DISCUSSION
In this study, the prevalence and severity of anemia in pregnant women were examined in relation to Complete Blood Count (CBC) results. 80% of the samples had Hemoglobin (Hb) levels between 10-11 g/dL, which is considered anemia in pregnancy (less than 11 g/dL)1. No sample had Hb levels above 11 g/dL; thus, a high rate of mild anemia in the study population.
This implies anemia remains a large public health issue among pregnant women in this region. It also implies nutritional deficiencies, reduced iron intake, and physiological pregnancy changes that augment iron requirements. Iron requirements nearly double in pregnancy to accommodate expanded maternal blood volume and fetal development. Failing to address these requirements will lead to iron deficiency and anemia6.
To identify the type of anemia, red cell indices such as Corpuscular Volume (MCV), Mean Corpuscular Hemoglobin (MCH), and Mean Corpuscular Hemoglobin Concentration (MCHC) were measured in addition to hemoglobin. The outcomes were as follows: MCV: 77.77 FL. This is a low normal range of 80-96 FL. This is microcytic anemia, small red blood cells. MCH: 25.14 pg. This is lower than the normal reference, low hemoglobin per cell. MCHC: 29.6 g/dL. This is less than the normal range of 32-36 g/dL, hypochromic anemia. Pale red blood cells from low hemoglobin. These are the iron deficiency anemia (IDA) blood patterns, which are the leading cause of anemia in pregnancy globally. Decrease in MCV, MCH, and MCHC together ensures that iron deficiency is the leading cause of anemia among this group7.
High anemia prevalence in this study is in accordance with findings from both local and foreign sources. As stated by the National Nutrition Survey8, over 50% of pregnant women in Pakistan are anemic, with the highest prevalence occurring in resource-poor areas like Balochistan. The same was observed by some authors9, who found that the absence of iron supplementation, inadequate dietary diversity, and frequent pregnancies without proper spacing are the primary reasons for rural Pakistani women’s low iron stores at pregnancy onset. As per the WHO 2021, anemia is found in 36.5% of pregnant women worldwide, and much more so in low- and middle-income nations (LMICs) such as Pakistan. Our research reflects an international pattern and substantiates the necessity for focused intervention in high-risk groups.
There are several reasons why anemia is so prevalent within the study population: A woman’s body needs more iron when she is pregnant to help the fetus grow, make the placenta, and increase her blood volume. It can cause depletion and anemia if she doesn’t get enough iron.
If you don’t consume sufficient heme iron from meat, poultry, and fish, and consume large amounts of phytate-rich plant foods and tannin-rich foods, your body may not properly absorb iron. This results in insufficient iron availability.
Despite national iron-folic acid tablet programs during pregnancy, there is low compliance due to side effects, ignorance, and irregular antenatal check-ups10.
Pregnancy anemia has significant consequences. Maternal morbidity consists of postpartum hemorrhage, infections, and death. For the infant, anemia is linked with low birth weight, preterm birth, and poor cognitive development11.
This research highlights the importance of public health interventions in addressing anemia during pregnancy, particularly in low-resource settings such as Balochistan. Effective strategies include ensuring the availability and accessibility of iron and folic acid supplementation during antenatal care visits, promoting nutrition education to encourage the intake of iron-rich and vitamin C-enhancing foods for better absorption, and implementing routine hemoglobin screening and follow-up as part of standard antenatal care protocols.
CONCLUSION
The study demonstrates a high prevalence of iron deficiency anemia among pregnant women in Quetta, with most participants showing reduced hemoglobin and abnormal hematological indices (MCV, MCH, MCHC, and HCT). Anemia was most pronounced during the second trimester due to increased physiological iron demands. These findings highlight the role of poor nutrition, inadequate supplementation, and socioeconomic factors in anemia persistence. Strengthening routine antenatal screening, nutritional awareness, and access to iron-folic acid supplementation is essential to improve maternal health outcomes.
SIGNIFICANCE STATEMENT
Iron deficiency anemia is a major threat to maternal and fetal health in underserved regions. This study evaluates hemoglobin distribution and hematological parameters among pregnant women in Quetta, Balochistan. Findings reveal a high prevalence of microcytic hypochromic anemia due to poor dietary intake, insufficient supplementation, and socioeconomic constraints. This work emphasizes the need for routine antenatal screening, dietary awareness, and accessible micronutrient supplementation to improve maternal health outcomes, especially in resource-limited areas.
FINDING
This research was funded by ORIC, BUITEMS, Quetta, under (Grant No. 01/Research Projects/ORIC/BUITEMS/2011/323)
ACKNOWLEDGMENT
The authors thank all study participants and staff for their cooperation.
REFERENCES
- WHO, 2021. Anaemia in Women and Children. World Health Organization, Geneva, Switzerland.
- Balarajan, Y., U. Ramakrishnan, E. Ozaltin, A.H. Shankar and S.V. Subramanian, 2011. Anaemia in low-income and middle-income countries. Lancet, 378: 2123-2135.
- Pavord, S., J. Daru, N. Prasannan, S. Robinson, S. Stanworth and J. Girling, 2020. UK guidelines on the management of iron deficiency in pregnancy. Br. Soc. Haematol., 188: 819-830.
- Government of Pakistan and UNICEF, 2019. National Nutrition Survey 2018-Key Findings Report. UNICEF & Pakistan Bureau of Statistics, Islamabad, Pakistan, Pages: 48.
- Mizanur, R.M., A.S. Krull, R.M. Shafiur, K. Mikiko and N. Saki et al., 2016. Maternal anemia and risk of adverse birth and health outcomes in low- and middle-income countries: Systematic review and meta-analysis. Am. J. Clin. Nutr., 103: 495-504.
- Black, R.E., C.G. Victora, S.P. Walker, Z.A. Bhutta and P. Christian et al., 2013. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet, 382: 427-451.
- Kalaivani, K., 2009. Prevalence and consequences of anaemia in pregnancy. Indian J. Med. Res., 130: 627-633.
- Ali, S.A., Z. Abbasi, B. Shahid, G. Moin and K.M. Hambidge et al., 2020. Prevalence and determinants of anemia among women of reproductive age in Thatta Pakistan: Findings from a cross-sectional study. PLoS ONE, 15.
- Kabir, M.A., M. Mostafizur Rahman and M.N. Khan, 2022. Maternal anemia and risk of adverse maternal health and birth outcomes in Bangladesh: A nationwide population-based survey. PLoS ONE, 17.
- Peña-Rosas, J.P., L.M. De-Regil, M.N. Garcia-Casal and T. Dowswell, 2015. Daily oral iron supplementation during pregnancy. Cochrane Database Syst. Rev., 2015.
- Allen, L.H., 2000. Anemia and iron deficiency: Effects on pregnancy outcome. Am. J. Clin. Nutr., 71: 1280S-1284S.
How to Cite this paper?
APA-7 Style
Khalid,
H., Malik,
S.F., Iqbal,
F., Daud,
S. (2026). A Cross-Sectional Study on the Distribution of Hemoglobin Levels Among Pregnant Women in Quetta, Balochistan. Trends in Biological Sciences, 2(3), 239-245. https://doi.org/10.21124/tbs.2026.239.245
ACS Style
Khalid,
H.; Malik,
S.F.; Iqbal,
F.; Daud,
S. A Cross-Sectional Study on the Distribution of Hemoglobin Levels Among Pregnant Women in Quetta, Balochistan. Trends Biol. Sci 2026, 2, 239-245. https://doi.org/10.21124/tbs.2026.239.245
AMA Style
Khalid
H, Malik
SF, Iqbal
F, Daud
S. A Cross-Sectional Study on the Distribution of Hemoglobin Levels Among Pregnant Women in Quetta, Balochistan. Trends in Biological Sciences. 2026; 2(3): 239-245. https://doi.org/10.21124/tbs.2026.239.245
Chicago/Turabian Style
Khalid, Halima, Sobia Faisal Malik, Fatima Iqbal, and Shakeela Daud.
2026. "A Cross-Sectional Study on the Distribution of Hemoglobin Levels Among Pregnant Women in Quetta, Balochistan" Trends in Biological Sciences 2, no. 3: 239-245. https://doi.org/10.21124/tbs.2026.239.245

This work is licensed under a Creative Commons Attribution 4.0 International License.