Red Cell Distribution Width as a Diagnostic and Prognostic Marker in Hospitalized Pediatric Patients: A Pilot Study from Yemen
-
Omar A. Bawazir
Department of Paediatrics, College of Medicine and Health Sciences, Hadhramout University, Mukalla 50511, Yemen
Noor A. BinkroomDepartment of Paediatrics, College of Medicine and Health Sciences, Hadhramout University, Mukalla 50511, Yemen
Mohamed S. BaazabDepartment of Paediatrics, College of Medicine and Health Sciences, University of Aden, Khur Maksar, Yemen
Naela A. Al-NakhbiDepartment of Basic Medical Sciences, College of Medicine and Health Sciences, Hadhramout University, Mukalla 50511, Yemen
Lotfi S. Dahman

Clinical Biochemistry Unit, Department of Laboratory Medicine, College of Medicine and Health Sciences, Hadhramout University, Mukalla 50511, Yemen
Jalil I. AlezziDepartment of Paediatric, College of Medicine, University of Diyala, Diyala, Iraq
| Received 21 Oct, 2025 |
Accepted 21 May, 2026 |
Published 30 Sep, 2026 |
Background and Objective: Red cell distribution width (RDW) is a routinely reported parameter in the Complete Blood Count (CBC), traditionally used in the diagnosis of anemia. Recent studies indicate that RDW may also serve as a valuable diagnostic and prognostic marker in a range of diseases. Despite this growing evidence, the significance of RDW in pediatric populations, especially within resource-limited settings, remains insufficiently investigated. This study was aimed to assess the distribution of RDW among hospitalized pediatric patients and explore its association with different disease categories. Materials and Methods: This retrospective study included 143 pediatric admissions aged 1 month to 14 years at a tertiary care hospital in Yemen. The RDW values were categorized as normal (≤14.5%) or high (>14.5%). Cases were grouped by major disease systems (e.g., gastrointestinal, respiratory, hematological). Descriptive statistics and chi-square tests were used for analysis. The p-value <0.05 was considered statistically significant. Results: Elevated RDW was observed in 91 (63.6%) cases. The highest proportions were found in inflammatory (100.0%) and hematological (96.0%) diseases. High RDW was also common in endocrine (75.0%) and nervous system (68.4%) conditions. Gastrointestinal, respiratory, and infectious diseases showed nearly equal distribution of normal and high RDW. A significant association was found between RDW status and disease system (χ2 = 23.05, p = 0.006), while subcategory-level comparisons were not statistically significant. Conclusion: The RDW was frequently elevated in pediatric admissions, particularly in hematological and inflammatory diseases. Its association with specific disease systems suggests potential as a supportive diagnostic marker in pediatrics. Further prospective studies are needed to clarify the role of RDW, especially in settings where anemia and inflammation are common.
| Copyright © 2026 Bawazir et al. This is an open-access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. |
INTRODUCTION
Red cell distribution width (RDW) is a routinely reported parameter in the Complete Blood Count (CBC) that reflects the variation in Red Blood Cell (RBC) size, or anisocytosis1.
While traditionally used in the differential diagnosis of anaemia, recent research has expanded its utility to include diagnostic and prognostic roles in a wide range of clinical conditions, including cardiovascular, infectious, inflammatory, and hematologic diseases2-5.
In adult populations, elevated RDW has been associated with increased morbidity and mortality in a wide range of conditions, including cardiovascular disease, infections, chronic kidney disease, and sepsis6. This association is thought to be related to inflammation-induced disruption of erythropoiesis and shortened RBC survival, both of which increase RDW values7. Because of its accessibility, low cost, and inclusion in routine laboratory panels, RDW has been proposed as a potential diagnostic and prognostic marker in both inpatient and outpatient settings1.
In paediatrics, however, the clinical utility of RDW remains less well established. A limited number of studies have investigated its role in specific pediatric conditions, such as lower respiratory tract infections, febrile seizures, Kawasaki disease, and anaemia6,8. These studies suggest that RDW may correlate with disease severity and inflammatory response in children, similar to findings in adults. Nonetheless, there is a lack of research exploring RDW patterns across a broad spectrum of pediatric illnesses, particularly in diverse real-world hospital settings.
Pediatric patients frequently present with nonspecific symptoms such as fever, vomiting, or respiratory distress, which makes early differential diagnosis challenging. Identifying biomarkers that can support clinical reasoning and early diagnosis is crucial. In this context, RDW may provide valuable insights when interpreted alongside other clinical and laboratory findings.
Despite the growing body of evidence supporting the clinical relevance of RDW, its role in differentiating and predicting outcomes across a spectrum of pediatric diseases remains underexplored particularly in resource-limited settings such as Yemen, where pediatric admissions frequently involve respiratory, gastrointestinal, and hematologic disorders.
This study aims to examine RDW values across a cohort of hospitalized children diagnosed with various disease categories, including gastrointestinal, respiratory, hematologic, neurologic, infectious, renal, and inflammatory conditions. This may provide clinically meaningful insights into the potential diagnostic and prognostic utility of RDW in pediatric practice.
MATERIALS AND METHODS
Study design and setting: This cross-sectional pilot study was conducted at Mukalla Maternity and Children Hospital in Hadramout, Yemen. It included 143 pediatric patients aged between 1 month and 14 years, who were admitted to the general pediatric ward between January and August 2023.
Data collection: Data were collected retrospectively from patients’ medical records and included:
| • | Demographics: Age and sex | |
| • | Clinical diagnosis: Categorized by the affected body system (e.g., gastrointestinal, respiratory, haematological) |
Complete Blood Count (CBC) parameters: Haemoglobin (Hb), Mean Corpuscular Volume (MCV), Red Cell Distribution Width (RDW), White Blood Cell Count (WBC), and platelet count were determined using an automated hematology analyzer following standard hematological laboratory procedures9.
Variable definitions:
| • | Disease categories: Were grouped by organ/system involvement (e.g., respiratory system, haematology) and subcategories (e.g., bronchiolitis, sickle cell disease) | |
| • | RDW group: Based on RDW values, patients were classified as: |
| • | Normal RDW (≤14.5%) | ||
| • | High RDW (>14.5%) |
| • | Anemia group: Anemia was defined as haemoglobin <10.5 g/dL | |
| • | MCV Cut-off: MCV was interpreted based on age-adjusted pediatric references: |
| • | MCV cut-off = 70+age in years (for children 1-10 years) | ||
| • | MCV cut-off = 80 fL for children>10 years |
Data management and statistical analysis: Data were analyzed using IBM SPSS Statistics (IBM Corp., Armonk, NY, USA)10. The statistical analysis included:
| • | Descriptive statistics: (Frequencies, percentages, means, and standard deviations) to summarize demographic characteristics and laboratory parameters | |
| • | Cross-tabulation analyses: Of RDW groups across: |
| • | Major disease categories | ||
| • | Common diagnostic subcategories (e.g., pneumonia, sickle cell disease) |
| • | Graphical presentation: Using bar charts to illustrate: |
| • | Disease distribution | |
| • | Proportion of elevated RDW across different disease systems |
| • | Inferential analysis: Using the Chi-square (χ2) test to assess associations between RDW groups and disease categories/subcategories. A p-value<0.05 was considered statistically significant. |
Ethical considerations: Ethical approval for the study was obtained Committee, College of Medicine and Health Sciences, Hadhramout University. As a retrospective chart review, informed consent was not required. All patient data were anonymised to ensure confidentiality.
RESULTS
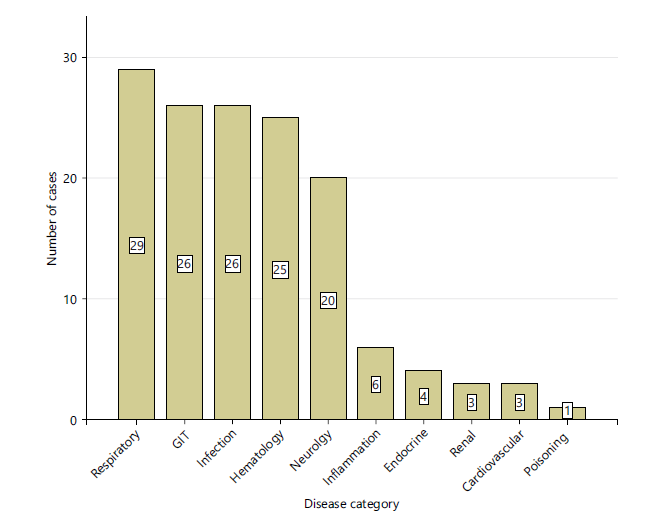
A total of 143 pediatric patients were included in this study. The mean age was 3.4 years (range: 1 month to 14 years). There were 85 males (59.4%) and 58 females (40.6%), with a male-to-female ratio of 1.5:1. The majority of patients were infants (1 month to <1 year, n = 46; 32.2%) and toddlers (1-3 years, n = 45; 31.5%), followed by preschool-age children (4-5 years, n = 21; 14.7%) (Table 1). The most common admitted patients were respiratory (29/143), GIT (26/143, infection (26/143), and haematology (25/143) (Fig. 1).
|
| Table 1: | Demographic characteristics of the study population (N = 143) | |||
| Characteristic | Number of patients (n) | Percentage |
| Sex | ||
| Male | 85 | 59.4 |
| Female | 58 | 40.6 |
| Age group | ||
| Infants (1 month-<1 year) | 46 | 32.2 |
| Toddlers (1-3 years) | 45 | 31.5 |
| Preschool (4-5 years) | 21 | 14.7 |
| School-aged (>5-14 years) | 31 | 21.7 |
| Total | 143 | 100 |
Among all admissions, 91 cases (63.6%) had elevated RDW values (>14.5%), while 52 cases (36.4%) had normal RDW values (Table 2). When analyzed by disease system, the highest proportions of elevated RDW were observed in:
| • | Inflammatory conditions: 6 out of 6 cases (100.0%) | |
| • | Hematological diseases: 24 out of 25 cases (96.0%) | |
| • | Endocrine diseases: 3 out of 4 cases (75.0%) | |
| • | Nervous system disorders: 13 out of 19 cases (65.0%) |
Besides, gastrointestinal (53.8%), respiratory (51.7%), and infectious diseases (53.8%) also showed nearly equal proportions of normal and high RDW. A Chi-square test was performed to assess the association between RDW status and disease systems. The test revealed a statistically significant association between inflammatory conditions, hematological diseases, endocrine diseases, and nervous system disorders with high RDW values (χ2 = 23.05, p = 0.006).
Table 3 shows the distribution of RDW status among pediatric respiratory diseases (n = 29).
| Table 2: | Distribution of RDW status across disease categories (N: 143) | |||
| RDW group | ||||
| Disease system | Normal RDW | High RDW | Total | |
| Cardiovascular | Count | 2 | 1 | 3 |
| % Within disease system | 66.70% | 33.30% | 100.00% | |
| % Within RDW group | 3.80% | 1.10% | 2.10% | |
| % Total | 1.40% | 0.70% | 2.10% | |
| Endocrine | Count | 1 | 3 | 4 |
| % Within disease system | 25.00% | 75.00% | 100.00% | |
| % Within RDW group | 1.90% | 3.30% | 2.80% | |
| % Total | 0.70% | 2.10% | 2.80% | |
| GIT | Count | 12 | 14 | 26 |
| % Within disease system | 46.20% | 53.80% | 100.00% | |
| % Within RDW group | 23.10% | 15.40% | 18.20% | |
| % Total | 8.40% | 9.80% | 18.20% | |
| Haematology | Count | 1 | 24 | 25 |
| % Within disease system | 4.00% | 96.00% | 100.00% | |
| % Within RDW group | 1.90% | 26.40% | 17.50% | |
| % Total | 0.70% | 16.80% | 17.50% | |
| Infection | Count | 12 | 14 | 26 |
| % Within disease system | 46.20% | 53.80% | 100.00% | |
| % Within RDW group | 23.10% | 15.40% | 18.20% | |
| % Total | 8.40% | 9.80% | 18.20% | |
| Inflammation | Count | 0 | 6 | 6 |
| % Within disease system | 0.00% | 100.00% | 100.00% | |
| % Within RDW group | 0.00% | 6.60% | 4.20% | |
| % Total | 0.00% | 4.20% | 4.20% | |
| Nervous system | Count | 7 | 13 | 20 |
| % Within disease system | 35.00% | 65.00% | 100.00% | |
| % Within RDW group | 13.50% | 14.30% | 14.00% | |
| % Total | 4.90% | 9.10% | 14.00% | |
| Poisoning | Count | 1 | 0 | 1 |
| % Within disease system | 100.00% | 0.00% | 100.00% | |
| % Within RDW group | 1.90% | 0.00% | 0.70% | |
| % Total | 0.70% | 0.00% | 0.70% | |
| Renal system | Count | 2 | 1 | 3 |
| % Within disease system | 66.70% | 33.30% | 100.00% | |
| % Within RDW group | 3.80% | 1.10% | 2.10% | |
| % Total | 1.40% | 0.70% | 2.10% | |
| Respiratory disease | Count | 14 | 15 | 29 |
| % Within disease system | 48.30% | 51.70% | 100.00% | |
| % Within RDW group | 26.90% | 16.50% | 20.30% | |
| % Total | 9.80% | 10.50% | 20.30% | |
| Total | Count | 52 | 91 | 143 |
| % Within disease system | 36.40% | 63.60% | 100.00% | |
| % Within RDW group | 100.00% | 100.00% | 100.00% | |
| % Total | 36.40% | 63.60% | 100.00% | |
| Red cell distribution width (RDW) | ||||
| Table 3: | Distribution of RDW status among pediatric respiratory disease admission (N: 29/143) | |||
| RDW group | |||
| Respiratory diseases | Normal RDW | High RDW | Total |
| Bronchiolitis | 8 (61.5%) | 5 (38.5%) | 13 |
| Viral-induced wheeze | 0 (0.00%) | 4 (100%) | 4 |
| Bronchial asthma | 1 (50%) | 1 (50%) | 2 |
| Pneumonia | 4 (50%) | 4 (50%) | 8 |
| Shortness of breath | 0 (0.00%) | 1 (100%) | 1 |
| Tonsillitis | 1 (100%) | 0 (0.00%) | 1 |
| Total | 14 | 15 | 29 |
| Red cell distribution width (RDW) | |||
| Table 4: | Distribution of RDW Status among pediatric GIT disease admission (N: 26/143) | |||
| RDW group | |||
| GIT | Normal RDW | High RDW | Total |
| Gastroenteritis | 10 (47.6%) | 11 (52.4%) | 21 |
| Abdominal pain | 1 (100%) | 0 (0.00%) | 1 |
| Hepatitis | 0 (0.00%) | 1 (100%) | 1 |
| Crohn's disease | 0 (0.00%) | 1 (100%) | 1 |
| Liver tumor | 1 (100%) | 0 (0.00%) | 1 |
| Malnutrition | 0 (0.00%) | 1 (100%) | 1 |
| Total | 12 | 14 | 26 |
| Red cell distribution width (RDW) | |||
| Table 5: | Distribution of RDW status among pediatric infectious diagnosed admission (N: 26/143) | |||
| RDW group | |||
| Infection | Normal RDW | High RDW | Total |
| Measles | 7 (46.7%) | 8 (53.3%) | 15 |
| Dengue fever | 1 (50%) | 1 (50%) | 2 |
| Upper respiratory infection | 2 (66.7%) | 1 (33.3%) | 3 |
| CMV | 0 (0.00%) | 1 (100%) | 1 |
| Fever of unknown origin | 2 (66.7%) | 1 (33.3%) | 3 |
| Whooping cough | 0 (0.00%) | 2 (100%) | 2 |
| Total | 12 | 14 | 26 |
Normal RDW was observed in 14 patients, while high RDW was found in 15 patients. Among bronchiolitis cases (n = 13), 8 patients (61.5%) had normal RDW and 5 patients (38.5%) had high RDW. All patients with viral-induced wheeze (n = 4) had high RDW (100%), with no cases showing normal RDW. In bronchial asthma (n = 2), 1 patient (50%) had normal RDW and 1 patient (50%) had high RDW. Similarly, pneumonia cases (n = 8) showed equal distribution: 4 patients (50%) had normal RDW and 4 patients (50%) had high RDW. A single case of shortness of breath (n = 1) had high RDW (100%), while a single tonsillitis case (n = 1) had normal RDW (100%).
Table 4 shows the distribution of RDW status among pediatric gastrointestinal diseases (n = 26). Normal RDW was observed in 12 patients, while high RDW was found in 14 patients. Among gastroenteritis cases (n = 21), 10 patients (47.6%) had normal RDW and 11 patients (52.4%) had high RDW. The single cases of hepatitis, Crohn's disease, and malnutrition had high RDW (100%), while, abdominal pain and liver tumor had normal RDW (100%).
Table 5 shows the distribution of RDW status among pediatric infectious diseases (n = 26). Normal RDW was observed in 12 patients, while high RDW was found in 14 patients. Among measles cases (n = 15), 7 patients (46.7%) had normal RDW and 8 patients (53.3%) had high RDW. In dengue fever (n = 2), 1 patient (50%) had normal RDW and 1 patient (50%) had high RDW. For upper respiratory infection and fever of unknown origin (n = 3), 2 patients (66.7%) had normal RDW and 1 patient (33.3%) had high RDW. Whooping cough (n = 2) had high RDW (100%).
Table 6 shows the distribution of RDW status among pediatric hematological diseases (n = 25). Normal RDW was observed in 1 patient, while high RDW was found in 24 patients. All cases of immune thrombocytopenic purpura (n = 2), thalassemia (n = 3), anemia (n = 5), megaloblastic anaemia (n = 1), platelet count defect (n = 1), myelodysplastic syndrome (n = 1), and haemolytic anemia (n = 1) had high RDW (100%). Among sickle cell anemia cases (n = 11), 1 patient (9%) had normal RDW and 10 patients (91%) had high RDW.
| Table 6: | Distribution of RDW status among pediatric haematology diagnosed admission (N: 25/143) | |||
| RDW group | |||
| Haematology | Normal RDW | High RDW | Total |
| Immune thrombocytopenic purpura | 0 (0.00%) | 2 (100%) | 2 |
| Sickle cell anaemia | 1 (9%) | 10 (91%) | 11 |
| Thalassemia | 0 (0.00%) | 3 (100%) | 3 |
| Anemia for investigation | 0 (0.00%) | 5 (100%) | 5 |
| Megaloblastic anaemia | 0 (0.00%) | 1 (100%) | 1 |
| Platelet function defect | 0 (0.00%) | 1 (100%) | 1 |
| Myelodysplastic syndrome | 0 (0.00%) | 1 (100%) | 1 |
| Haemolytic anaemia | 0 (0.00%) | 1 (100%) | 1 |
| Total | 1 | 24 | 25 |
| Table 7: | Distribution of RDW status among pediatric neurology diagnosed admission (N: 20/143) | |||
| RDW group | |||
| Nervous system | Normal RDW | High RDW | Total |
| Febrile convulsion | 4 (57%) | 3 (43%) | 7 |
| Epilepsy | 1 (33.3%) | 2 (66.7%) | 3 |
| Guillain Barr syndrome | 0 (0.00%) | 2 (100%) | 2 |
| Encephalopathy | 1 (100%) | 0 (0.00%) | 1 |
| Hydrocephalus | 0 (0.00%) | 2 (100%) | 2 |
| Birth asphyxia | 0 (0.00%) | 1 (100%) | 1 |
| Cerebral palsy | 0 (0.00%) | 3 (100%) | 3 |
| Meningitis | 1 (100%) | 0 (0.00%) | 1 |
| Total | 7 | 13 | 20 |
Table 7 shows the distribution of RDW status among pediatric neurological diseases (n = 20). Normal RDW was observed in 7 patients, while high RDW was found in 13 patients. Among febrile convulsion cases (n = 7), 4 patients (57%) had normal RDW and 3 patients (43%) had high RDW. In epilepsy (n = 3), 1 patient (33.3%) had normal RDW and 2 patients (66.7%) had high RDW. All cases of Guillain–Barré syndrome (n = 2), hydrocephalus (n = 2), birth asphyxia (n = 1), and cerebral palsy (n = 3) had high RDW (100%). Whereas, cases of encephalopathy (n = 1) and meningitis (n= 1) showed normal RDW (100%).
DISCUSSION
This study evaluated the distribution of red cell distribution width (RDW) in hospitalized pediatric patients across multiple disease systems. Elevated RDW (>14.5%) was observed in nearly two-thirds of cases (63.6%), indicating a high prevalence of anisocytosis. The highest proportions were found in hematological (96.0%) and inflammatory (100.0%) conditions, consistent with prior evidence linking RDW to iron deficiency anemia, thalassemia, and immune thrombocytopenia1,11.
In respiratory diseases, all children with viral-induced wheeze (4/4, 100%) exhibited elevated RDW compared with 50% (13/25) of bronchiolitis cases. Although not statistically significant (χ2 = 6.67, p = .247), the consistent elevation in viral-induced wheeze suggests possible systemic stress or inflammation. Elevated RDW has similarly been associated with poor outcomes in pediatric respiratory illnesses12,13, warranting further study in larger cohorts.
Both whooping cough cases showed high RDW. The combination of persistent cough, elevated RDW, normal ESR, and lymphocytosis may serve as a useful clinical clue for pertussis, particularly in resource-limited settings. To date, no studies have specifically examined this relationship, highlighting an area for future research.
In hematological disorders, elevated RDW was expected. Sickle cell disease typically demonstrates marked anisocytosis due to reticulocytosis and abnormal morphology, with higher RDW correlating with disease severity and complications2,14. In thalassemia, RDW varies by subtype but is often markedly elevated in thalassemia major15,16. All patients with hemophagocytic lymphohistiocytosis (6/6, 100%) also had elevated RDW, supporting findings by Xi et al. that RDW may help distinguish HLH from other systemic inflammatory diseases.
Endocrine and neurological conditions showed elevated RDW in 75.0% and 68.4% of cases, respectively. In diabetes, chronic hyperglycemia and oxidative stress can increase RDW, which has been associated with complications and prognosis17,18. Interestingly, both diabetic ketoacidosis cases in this cohort survived despite elevated RDW, contrasting with adult studies that reported higher mortality18. This discrepancy may reflect age-related differences or a small sample size.
Gastrointestinal and respiratory groups demonstrated a mixed RDW distribution (~50% elevated), reflecting the heterogeneity of conditions, ranging from mild infections to chronic inflammatory or malabsorptive states such as Crohn’s disease, hepatitis, or malnutrition.
A chi-square test confirmed a significant association between RDW status and disease system (χ2 = 23.05, p = .006), though subgroup comparisons lacked significance, likely due to small sample sizes.
Interpretation of elevated RDW in pediatric patients is particularly challenging in resource-limited settings with high baseline rates of iron deficiency anemia. Nevertheless, elevated RDW among non-anemic patients suggests it may also reflect systemic inflammation or oxidative stress beyond nutritional causes.
In summary, RDW is a low-cost, widely available marker that demonstrates variability across pediatric disease systems and may provide clinical value for diagnosis and risk stratification, particularly in settings where advanced laboratory tests are limited.
In summary, findings suggest that elevated RDW is common among hospitalized pediatric patients and may serve as a useful marker of systemic inflammation, oxidative stress, or underlying hematologic disorders. While RDW alone cannot replace specific diagnostic tests, its routine availability and low cost make it a potentially valuable tool for early risk stratification in resource-limited settings. Future prospective studies with larger sample sizes and inclusion of iron studies or inflammatory markers are needed to further validate these observations and explore the utility of RDW in specific pediatric disease contexts.
The study was limited by a small sample size, particularly in disease subgroups, and a cross-sectional design that precluded causal inferences or tracking RDW changes over time. Lack of confirmatory lab tests (e.g., ferritin, inflammatory markers) hindered differentiation between RDW elevations due to deficiency versus inflammation. Retrospective data collection may have introduced bias. Future prospective studies with larger cohorts and detailed biomarker analysis are needed to clarify RDW’s diagnostic and prognostic role in pediatric conditions.
CONCLUSION
This study shows that elevated red cell distribution width (RDW) is common in hospitalized children, especially those with haematological or inflammatory conditions like sickle cell disease, thalassemia, and whooping cough. Elevated RDW appears to reflect systemic stress, inflammation, or abnormal red blood cell production, even in non-anaemic patients. Due to its low cost and routine availability in blood tests, RDW may serve as a valuable tool for early risk assessment and diagnosis in pediatric care, particularly in settings with limited resources.
SIGNIFICANCE STATEMENT
This study highlights red cell distribution width (RDW) as a readily available, low-cost biomarker in pediatric patients. Elevated RDW was prevalent in hematological and inflammatory conditions, suggesting its potential for early diagnosis and risk stratification. In resource-limited settings like Yemen, routine RDW assessment may support clinical decision-making, guide further investigations, and improve pediatric care where advanced laboratory testing is scarce.
REFERENCES
- Salvagno, G.L., F. Sanchis-Gomar, A. Picanza and G. Lippi, 2015. Red blood cell distribution width: A simple parameter with multiple clinical applications. Crit. Rev. Clin. Lab. Sci., 52: 86-105.
- Yousefi, B., S. Sanaie, A.A. Ghamari, H. Soleimanpour, A. Karimian and A. Mahmoodpoor, 2020. Red cell distribution width as a novel prognostic marker in multiple clinical studies. Indian J. Crit. Care Med., 24: 49-54.
- Piriyakhuntorn, P., A. Tantiworawit, T. Rattanathammethee, C. Chai-Adisaksopha, E. Rattarittamrong and L. Norasetthada, 2018. The role of red cell distribution width in the differential diagnosis of iron deficiency anemia and non-transfusion dependent thalassemia patients. Hematol. Rep., 10.
- Lippi, G., G. Targher, M. Montagnana, G.L. Salvagno, G. Zoppini and G.C. Guidi, 2009. Relation between red blood cell distribution width and inflammatory biomarkers in a large cohort of unselected outpatients. Arch. Pathol. Lab. Med., 133: 628-632.
- Tonelli, M., F. Sacks, M. Arnold, L. Moye, B. Davis and M. Pfeffer, 2008. Relation between red blood cell distribution width and cardiovascular event rate in people with coronary disease. Circulation, 117: 163-168.
- Xu, H., S. Fu, W. Wang, Q. Zhang and J. Hu et al., 2016. Predictive value of red blood cell distribution width for coronary artery lesions in patients with Kawasaki disease. Cardiol. Young, 26: 1151-1157.
- Hu, Z.D., Y. Chen, L. Zhang, Y. Sun and Y.L. Huang et al., 2013. Red blood cell distribution width is a potential index to assess the disease activity of systemic lupus erythematosus. Clin. Chim. Acta, 425: 202-205.
- Marzouk, H., N. Mostafa, I. Khalifa, N. Badawi and N.I.M.F. Sabry, 2020. Red cell distribution width (RDW) as a marker of subclinical inflammation in children with familial Mediterranean fever. Curr. Rheumatol. Rev., 16: 298-303.
- Bain, B.J., S.M. Lewis and J.V. Dacie, 2016. Dacie and Lewis Practical Haematology. 12th Edn., Elsevier, Amsterdam, Netherlands, ISBN-13: 9780702069253, Pages: 600.
- Abd El Gawaad, E.H.A., H.S. Mohammad, T.H.M. Elkhatib and G.A. Khalil, 2019. Assessment of extracranial carotid arteries in acute ischemic stroke: Correlation with risk factors. Int. J. Clin. Exp. Neurol., 7: 1-6.
- Ramby, A.L., D.M. Goodman, E.L. Wald and S.L. Weiss, 2015. Red blood cell distribution width as a pragmatic marker for outcome in pediatric critical illness. PLoS ONE, 10.
- Çelik, E., S.F. Çelik, Ş. Güngör and A. Dursun, 2021. Impact of anaemia on the severity of acute bronchiolitis in infants. J. Nepal Paediatr. Soc., 41: 73-79.
- Kattamis, A., G.L. Forni, Y. Aydinok and V. Viprakasit, 2020. Changing patterns in the epidemiology of β‐thalassemia. Eur. J. Haematol., 105: 692-703.
- Keikhaei, B., M. Bahadoram, M.R. Mahmoudian-Sani and S. Bahadoram, 2021. Red cell distribution width as a differential parameter between iron deficiency anemia and α-thalassemia: An empirical approach. Pediatr. Hematol. Oncol. Immunopathol., 20: 156-157.
- Moustafa, A.N., H.M. Moness and M.W.E. Ali, 2023. Red cell distribution width as a prognostic marker for complications of community-acquired pneumonia in children: A comparison with Proadrenomedullin and Copeptin. BMC Pulm. Med., 23.
- Jing, R., B. Yu, C. Xu, Y. Zhao, H. Cao, W. He and H. Wang, 2024. Association between red cell distribution width-to-albumin ratio and prognostic outcomes in pediatric intensive care unit patients: A retrospective cohort study. Front. Pediatr., 12.
- Ma, Y., S. Li, A. Zhang, Y. Ma and Y. Wan et al., 2021. Association between red blood cell distribution width and diabetic retinopathy: A 5-year retrospective case-control study. J. Ophthalmol., 2021.
- Dai, H., X. Su, H. Li and L. Zhu, 2020. Association between red blood cell distribution width and mortality in diabetic ketoacidosis. J. Int. Med. Res., 48.
How to Cite this paper?
APA-7 Style
Bawazir,
O.A., Binkroom,
N.A., Baazab,
M.S., Al-Nakhbi,
N.A., Dahman,
L.S., Alezzi,
J.I. (2026). Red Cell Distribution Width as a Diagnostic and Prognostic Marker in Hospitalized Pediatric Patients: A Pilot Study from Yemen. Trends in Biological Sciences, 2(3), 255-264. https://doi.org/10.21124/tbs.2026.255.264
ACS Style
Bawazir,
O.A.; Binkroom,
N.A.; Baazab,
M.S.; Al-Nakhbi,
N.A.; Dahman,
L.S.; Alezzi,
J.I. Red Cell Distribution Width as a Diagnostic and Prognostic Marker in Hospitalized Pediatric Patients: A Pilot Study from Yemen. Trends Biol. Sci 2026, 2, 255-264. https://doi.org/10.21124/tbs.2026.255.264
AMA Style
Bawazir
OA, Binkroom
NA, Baazab
MS, Al-Nakhbi
NA, Dahman
LS, Alezzi
JI. Red Cell Distribution Width as a Diagnostic and Prognostic Marker in Hospitalized Pediatric Patients: A Pilot Study from Yemen. Trends in Biological Sciences. 2026; 2(3): 255-264. https://doi.org/10.21124/tbs.2026.255.264
Chicago/Turabian Style
Bawazir, Omar, A., Noor A. Binkroom, Mohamed S. Baazab, Naela A. Al-Nakhbi, Lotfi S. Dahman, and Jalil I. Alezzi.
2026. "Red Cell Distribution Width as a Diagnostic and Prognostic Marker in Hospitalized Pediatric Patients: A Pilot Study from Yemen" Trends in Biological Sciences 2, no. 3: 255-264. https://doi.org/10.21124/tbs.2026.255.264

This work is licensed under a Creative Commons Attribution 4.0 International License.