Spatial Epidemiology and Risk Factors Associated with Surficial Fungal Infection in Schoolchildren of North Pakistan
-
Azhar Hussain


Department of Agriculture and Food Technology Karakoram International University Gilgit, Gilgit-Baltistan, Pakistan
Maisoor Ahmad NafeesDepartment of Animal Science Karakoram International University Gilgit, Gilgit-Baltistan, Pakistan
Ghulam AbbasDepartment of Animal Science Karakoram International University Gilgit, Gilgit-Baltistan, Pakistan
Saif ud DinDepartment of Animal Science Karakoram International University Gilgit, Gilgit-Baltistan, Pakistan
| Received 16 Oct, 2025 |
Accepted 18 Jun, 2026 |
Published 30 Sep, 2026 |
Background and Objective: Superficial fungal infections (SFIs) pose a significant public health challenge, particularly among school-age children worldwide, including in Pakistan, with a specific focus on Gilgit-Baltistan. The objective of this study was to investigate the spatial epidemiology of SFIs in various schools and identify associated risk factors, to implement evidence-based strategies in fragile regions. Materials and Methods: A descriptive, geostatistical, and GIS mapping approach was used in this research. Five valleys in Gilgit-Baltistan were selected, with a total of 50 schools, from which 10 were randomly chosen per valley. A total of 850 primary schoolchildren were assessed for SFI infections, and the types of fungal species were determined. To analyze risk factors, infected students were randomly selected and surveyed using a structured questionnaire. Thematic maps were created using ArcMap 10.8 with ArcGIS software’s Spatial Analyst function, employing the Inverse Distance Weight (IDW) interpolation method. Results: The study revealed varying spatial patterns of SFI prevalence across the region, with prevalence ranging from 60 to 80% and incidence from 14.98 to 26.42%. The most common species were T. faciei, T. capitis, and T. corporis, with T. manuum being the least frequent. Geo-statistical analysis showed moderate spatial dependency for overall SFI prevalence (67.51) and incidence (72.81), with stronger dependencies observed for specific species. Risk factors identified included joint family systems, pit latrines, pet interactions, sharing personal items, and low socioeconomic status. Conclusion: This study highlights the urgent need for health education programs to reduce SFI prevalence and mitigate its long-term health and socioeconomic impacts among schoolchildren.
| Copyright © 2026 Hussain et al. This is an open-access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. |
INTRODUCTION
Gilgit-Baltistan is struggling with various health challenges, including cancer, heart disease, hepatitis, and infections such as COVID-191, malaria, typhoid fever, and tuberculosis. Surficial fungal infections (SFI), which also pose a substantial threat to public health and occur in School children, receive significantly less attention.
Consequently, there is a dearth of data regarding the burden of fungal diseases in the region. SFI is the most common and emerging public health issue worldwide, including in Pakistan. According to different reports SFI have been found in the last decades to affect 20-25% of the world’s population. These infection percentages vary within couriers, even within regions within countries, making them one of the most frequent forms of infection1. According to GAFFI (Global Action for Fungal Infection) estimated that over 300 million people of all ages suffer from a serious fungal infection each year globally and 1.5 million individuals die due to fungal infection. One of the main reasons is SFI is the most neglected issue in many developing countries2. According to CDC 2020 reports, fungi infections generate high rates of morbidity and mortality approximately about 1 billion people worldwide have cutaneous fungal infections of the skin, hair, and nails3. Patients who also have other coexisting clinical disorders, such as immunological malfunction, chemotherapy, cancer, and long-term chronic diseases, have considerably greater rates of morbidity and mortality from infection. One of the most vulnerable groups of our society to SFI is School children’s and reported many parts of world4. School-aged children are more susceptible to fungal infections due to factors such as inadequate personal cleanliness, frequent human interaction, unhygienic living conditions, crowding, and low socioeconomic position. The frequency of superficial skin fungal infections among kids in underdeveloped countries ranges between 20% and 90%4. In Gilgit-Baltistan the Multiple Indicators, Cluster Survey conducted in 2016-17 indicated that two out of ten children under the age of five are underweight (19.4%) while 5.6% are severely underweight. Almost half of the children under five (46.2%) are stunted; this could be linked to the non-availability of a balanced diet and the low nutritional status of mothers. Along with the nutrition, deficiency faced by the children, SFI also triggers and create health complications.
Tinea capitis, the most frequently occurring SFI, is the dominant species affecting children under the age of twelve. In impoverished nations, skin infections affect 21-87% of children. In Nigeria, prevalence rates ranged from 3.4 to 55.1%, and the severity of illness varied according to age, gender, geographical area, behaviour, and hygienic conditions. SFI is a significant health risk for schools, along with its epidemiology has evolved due to human movement patterns, pharmacological therapy, lifestyle, and socioeconomic status.
Geographic Information Systems (GIS) have become indispensable tools in spatial analysis and mapping, offering a robust framework for understanding and managing spatial data. The GIS integrates hardware, software, and data to facilitate the analysis of geographic phenomena, enabling users to visualize, interpret, and analyze spatial patterns and relationships in various contexts, from urban planning to environmental management. One of the critical roles of GIS in spatial analysis is its capacity to support decision-making processes by transforming raw geographical data into actionable insights. The GIS enables users to analyze patterns, trends, and distributions of phenomena across space, which is essential in fields like urban planning, resource management, and public health. By mapping variables such as population density, land use, and environmental risks, GIS allows policymakers to identify areas that require intervention or development5,6. This is the first study to assess epidemiology and highlight risk factors for SFI to fill the gaps regarding SFI in School children.
MATERIALS AND METHODS
Study area and duration: The present research on spatial epidemiology and risk factors associated with School children was carried out in District Skardu, Gilgit-Baltistan, Pakistan (Fig. 1).

|
Survey: For these purposes five valleys, fifty schools and ten schools (March-June 2024), each valley was randomly selected. Within each school primary School children s were used to assess SFI infection and types of SFI species by using following formulas7,8. Disease prevalence in valley wises was calculated as:
The percentage of occurrence of surficial fungal infection of each class was calculated by using the formula:
| OCC/C (%) | = | Occurrence percentage per class | |
| N.SFI/C | = | Number of surficial infected students per class | |
| T.N.S.C | = | Total number of students in a class |
Body part infected by SFI was calculated:
| F (%) | = | Frequency percentage | |
| NBPI | = | Number of cases of body part infected | |
| TNC | = | Total number of cases |
|
| Table 1: | Dominant risk factor associated with SFI in School children of district Skardu | |||
| Risk factors | Details |
| RF1 | Joint family |
| RF2 | Pit latrine facility |
| RF3 | Play with pets |
| RF4 | Sharing materials (Comb, head, brush, cloth and socks) |
| RF5 | Playing games with muds |
| RF6 | Sharing towel with family |
| RF7 | Frequently body contact with school mats |
| RF8 | No knowledge of personnel hygiene |
| RF9 | Over crowding |
| RF10 | Low socio economic condition |
| RF11 | Family history of skin infection |
| RF12 | Bathing twice a week |
SFI spatial GIS distribution: Spatial distribution analysis of surficial fungal infection and respective fungal species was mapped using GIS. A database file (dbf) containing X and Y coordinates about the sampling site was established. A shape file (vector data) outlining the selected district Skardu, was created in ArcMap 10.8. In the project window, the DBF file was opened, with the X-field representing X-coordinates and the Y-field representing Y-coordinates. The Z field was utilized for SFI prevalence, incidence, and respective fungal species of each district. The shape file for the districts was also opened from the 'surface menu' of ArcMap spatial analyst. The interpolation method applied was inverse distance weight (IDW). The model selected for this study is the aspherical model, which has the following definition:
 |
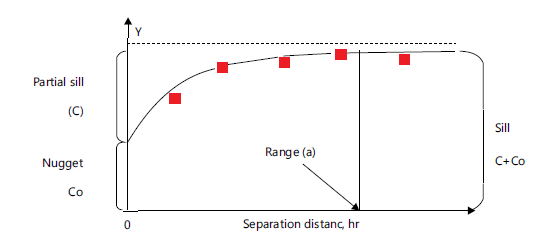
Spatial dependence (SDP %) was designed as described9,10 and is agreed by expression:
For the spherical semivariogram: SDP Spherical (%); ≤25% strong spatial dependence; 25%<SPD (%) ≤75% moderate spatial dependence and ≥75% weak spatial dependence (Fig. 2).
Risk factors of surficial fungal infection: This study was based on primary data collected from SFI infected students selected during personnel inspection during a school visit. From each student personal interview was conducted to find out the dominant risk factor of SFI prevalence mentioned in Table 1.
Statistical analysis: An analysis of variance (ANOVA) was performed to determine the mean difference within the valley by using Statistical Package (Statistix 8.1)11. Geostatistical Analysis was performed by using Arc GIS software 10.7 for spatial analysis, semivariogram, trend analysis, and GIS maps12.
RESULTS
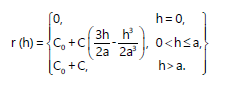
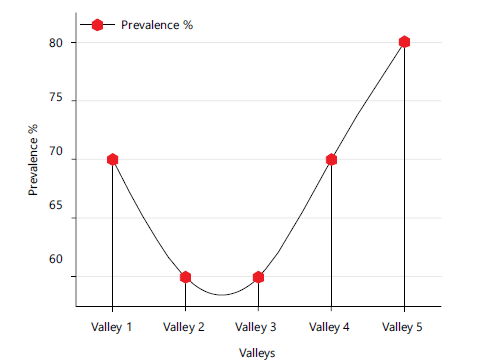
Superficial fungal infections are common in all age groups of people but the most common and highly vulnerable groups is school going children. In the current study, SFI prevalence, incidence and respective fungal species in different body parts ware studies. For this purposes, a comprehensive survey was carried in during the year 2023-24 in District Skardu, Gilgit-Baltistan Pakistan. Geographic Information System (GIS) was applied for preparation of SFI distribution map from data obtained during field survey. Results showed that SFI prevalence and incidence ranged from 60.0 to 80.0% and 14.98-26.42% while high prevalence and incidence was recorded in valley 5 and valley 4 (Fig. 3-4). Descriptive statistics was applied to know species was significant and non-significant between valleys. Result indicates that the means of three replicates in each column followed by the same letter are not significantly different at LSD test (p≤0.05). The mean occurrence of fungal species T. faciei (48.11±16.77) was found higher followed by T. capitis (13.10±7.21) and T. corporis (12.30±10.07), respectively (Table 2).
Geostatistical analysis: Semivariogram calculation revealed the possible spatial patterns of the various SFI parameters, and the best model to capture these spatial patterns was identified. The nugget effect (Co), sill (Co+C), and range of incidence for each parameter were recorded. The spatial dependencies (nugget/sill ratio) were discovered to be connected to the degree of correlation among each point of sampling and expressed in percentages.
| Table 2: | Assessment of different surficial fungal infection in school going children in district Skardu | |||
| SFI | Tinea capitis(Head) | Tinea faciei(Face) | Tinea corporis(Trunk) | Tinea unguium(Nail) | Tinea manuum(Hand) | Tinea pedis(Feet) |
| V1 | 25.58±19.24a | 20.27±16.59b | 29.32±16.28a | 7.06±9.24ab | 00.00±0.00c | 18.32±15.04a |
| V2 | 13.08±6.30ab | 51.80±14.23a | 9.13±6.43b | 10.70±7.94a | 7.25 ±5.62a | 11.71±6.04ab |
| V3 | 8.72±4.17b | 50.30±10.91a | 11.10±5.85b | 7.18A±4.32b | 4.91±3.31ab | 7.97±5.86ab |
| V4 | 8.56±8.40b | 52.34±26.99a | 9.52±3.54b | 5.43±6.12ab | 5.23±5.06ab | 7.05±5.77b |
| V5 | 9.57±12.04b | 65.84±12.80a | 2.44±5.11c | 3.04±3.73b | 2.44±3.68bc | 11.91±10.36ab |
| Mean | 13.1 | 48.11 | 12.3 | 6.68 | 3.96 | 11.39 |
| S.D | 7.21 | 16.77 | 10.07 | 2.8 | 2.79 | 4.44 |
| C.V | 55.03 | 34.87 | 81.9 | 41.9 | 70.56 | 38.99 |
| The values represent means of three replications and ±SD; the means with different letters/letter is statistically significant at p<0.05 | ||||||
|
|
| Table 3: | Geostatistical parameters for surficial fungal disease in district Skardu | |||
| SFI prameter | Model | Range (m) | N (Co) | PS (C) | S (Co+C) | N/S ratio | SDI % | Class |
| Prevalence | Gaussian | 256.3 | 1.141 | 0.555 | 1.69 | 0.657 | 67.51 | M |
| Incidence | Gaussian | 80 | 0.699 | 0.273 | 0.96 | 0.721 | 72.81 | M |
| Tinea capitis | Gaussian | 146.79 | 0.861 | 0.16 | 1.02 | 0.844 | 84.41 | W |
| Tinea faciei | Gaussian | 349.52 | 1.152 | 0.025 | 1.17 | 0.982 | 98.24 | W |
| Tinea corporis | Gaussian | 291.73 | 1.1 | 0.173 | 1.27 | 0.941 | 94.17 | W |
| Tinea unguium | Gaussian | 73.93 | 0.084 | 1.422 | 1.5 | 0.056 | 5.67 | S |
| Tinea manuum | Gaussian | 75.37 | 0.179 | 0.69 | 0.87 | 0.205 | 20.57 | S |
| Tinea pedis | Gaussian | 389.07 | 1.089 | 0.132 | 1.21 | 0.9 | 90 | W |
| N: Nugget, PS: Partial sill Sill; N/S ratio: [N/(N+PS) ans SD: Spatial dependence | ||||||||
The spatial dependent variables were classified as strongly spatially dependent if the ratio was 75%12,13. For SFI, disease prevalence and incidence had a moderate spatial dependence with a ratio 67.51 and 72.81% while the species-wise; T. capitis T. faciei T. corporis T. unguium T. manuum and T. pedis were classified as weak to strong spatially dependent with a ratio of 84.41, 98.24, 94.17, 5.67, 20.57, 20.57and 90.00%) % respectively (Table 3).
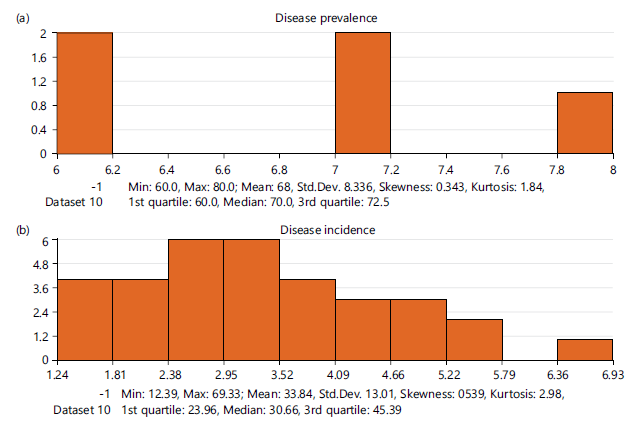
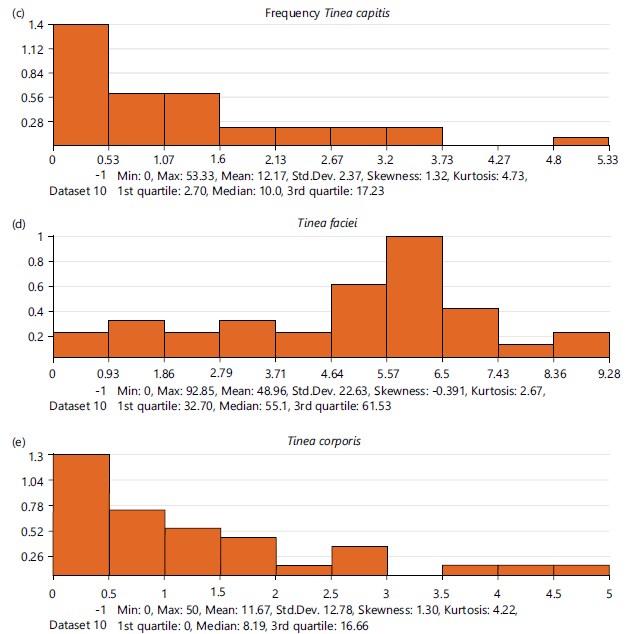
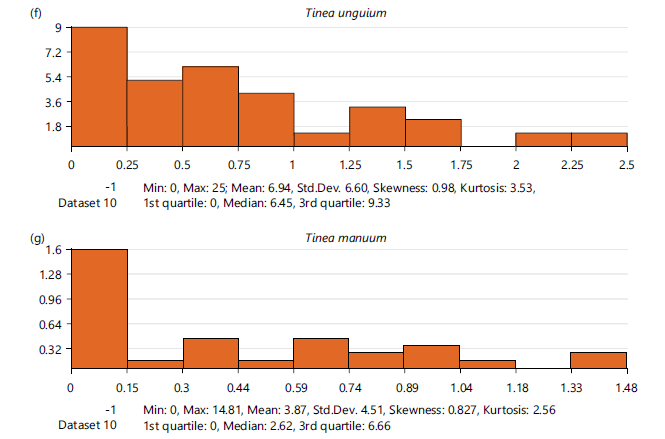
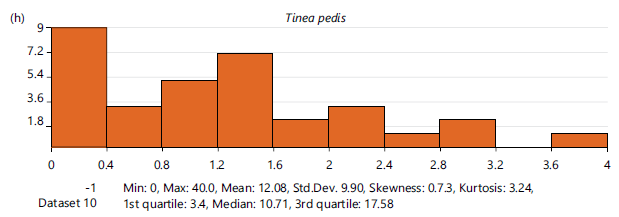
Histogram analysis: The results presented in Fig. 5 (a-h) illustrate the distribution and frequency patterns of superficial fungal infections (SFI), including overall prevalence, incidence, and species-specific occurrence in District Skardu. Figure 5a shows the overall disease prevalence, which ranged from 60.0% to 80.0%, with a mean value of 68% (±8.36). The median (70.0%) and quartile distribution indicate a moderately high burden of disease across the sampled population. The slight positive skewness (0.343) suggests that higher prevalence values were somewhat more frequent. Figure 5b presents disease incidence, with values ranging from 12.39 to 69.33 and a mean of 33.84 (±13.01). The distribution shows moderate variability and a positive skew (0.539), indicating occasional higher incidence rates in certain groups. Species-specific analysis reveals distinct patterns. In Fig. 5c, Tinea capitis exhibited a mean frequency of 12.17 with a high positive skewness (1.32), indicating that most cases were clustered at lower values with a few high outliers. Similarly, Tinea corporis (Fig. 5e) showed a mean of 11.67 (±12.78) and strong positive skewness (1.30), suggesting uneven distribution. In contrast, Tinea faciei (Fig. 5d) demonstrated a relatively higher mean frequency (48.96 ±22.63) with slight negative skewness (-0.391), indicating a more balanced spread of cases across the population. Lower frequencies were observed for Tinea unguium (Fig. 5f), Tinea manuum (Fig. 5g), and Tinea pedis (Fig. 5h), with mean values of 6.94, 3.87, and 12.08, respectively. These infections also displayed positive skewness, indicating that most observations were concentrated at lower frequencies with occasional higher values. Overall, the findings suggest that while overall SFI prevalence is high, individual fungal infections vary considerably in their distribution patterns, reflecting differences in transmission dynamics, environmental factors, and host susceptibility.
|
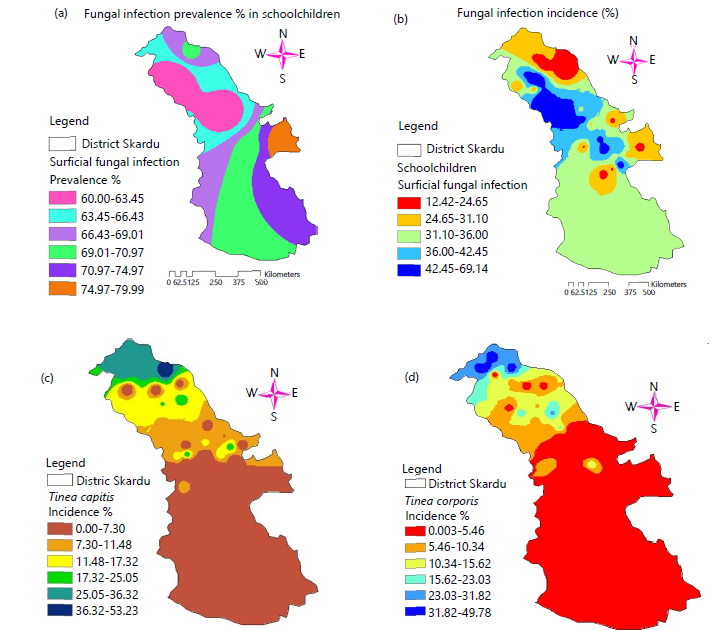
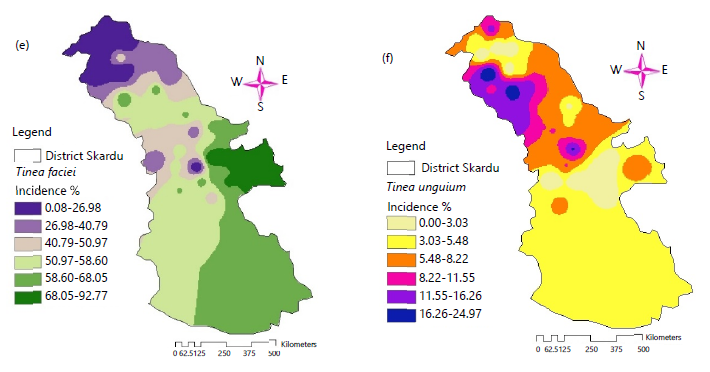
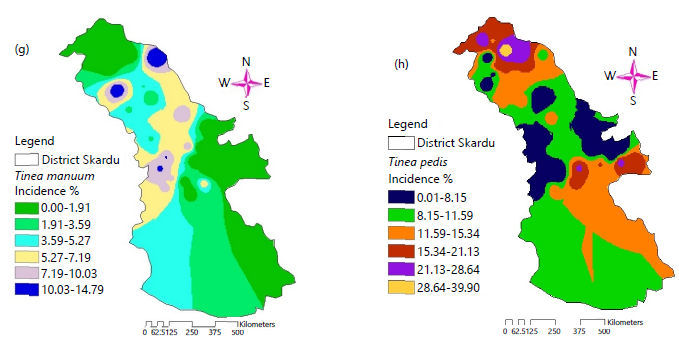
GIS mapping: The interpolation maps of SFI variables allowed us to visually understand the spatial distribution pattern in the study site. Fig. 6(a-h) presents the spatial distribution patterns of superficial fungal (SFI), including overall prevalence, incidence, and species-specific occurrence among School children in District Skardu. These maps provide important insights into the geographic clustering and variability of infections across different locations. Figure 6a illustrates the spatial distribution of overall SFI prevalence, showing that the burden of infection is not uniformly distributed.
|
Certain areas exhibit higher prevalence, indicating localized hotspots where environmental and socio-hygienic conditions may favour fungal growth and transmission. In contrast, some regions demonstrate comparatively lower prevalence, suggesting better hygiene practices or less favourable conditions for fungal proliferation. Figure 6b represents disease incidence, which also varies spatially. With higher incidence indicate active transmission zones, where new cases are frequently emerging. This uneven distribution highlights the role of population density, school environment, and behavioural factors in influencing disease spread. The species-specific maps (Fig. 6c-h) further reveal distinct spatial trends. Tinea capitis (Fig. 6c) shows clustering in selected suggesting close-contact transmission among children. Tinea faciei (Fig. 6d) appears more widely distributed, reflecting its relatively common occurrence. Tinea corporis (Fig. 6e) demonstrates moderate clustering, possibly linked to environmental exposure and personal hygiene. Lower-frequency infections such as Tinea unguium (Fig. 6f), Tinea manuum (Fig. 6g), and Tinea pedis (Fig. 6h) show scattered and less dense spatial patterns. However, certain localized pockets still exhibit higher concentrations, indicating specific risk factors such as shared facilities, moisture exposure, or inadequate sanitation. Overall, the spatial analysis indicates that SFI distribution is highly heterogeneous across District Skardu. The presence of distinct hotspots emphasizes the need for targeted public health interventions, including hygiene education, early diagnosis, and localized treatment strategies to effectively control and prevent the spread of fungal infections among School children.
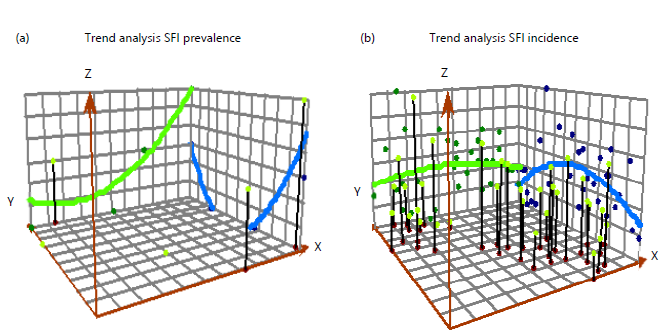
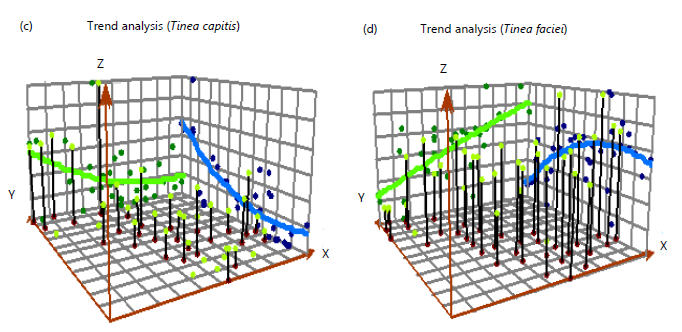
Trend analysis: To reduce the impacts of total trends on the local semi-variant analysis process and more accurately simulate short-range random variation, trend surface analysis was performed in order to obtain SFI trends. Based on the IDW interpolation, the trend analyses of SFI prevalence, incidence and respective. The trend analysis of superficial fungal infections in District Skardu, encompassing overall prevalence, incidence and species-specific trends, is shown in Fig. 7(a-h).
Certain areas exhibit higher prevalence, indicating localized hotspots where environmental and socio-hygienic conditions may favour fungal growth and transmission. In contrast, some regions demonstrate comparatively lower prevalence, suggesting better hygiene practices or less favourable conditions for fungal proliferation. Figure 6b represents disease incidence, which also varies spatially. With higher incidence indicate active transmission zones, where new cases are frequently emerging. This uneven distribution highlights the role of population density, school environment, and behavioural factors in influencing disease spread. The species-specific maps (Fig. 6c-h) further reveal distinct spatial trends. Tinea capitis (Fig. 6c) shows clustering in selected suggesting close-contact transmission among children. Tinea faciei (Fig. 6d) appears more widely distributed, reflecting its relatively common occurrence. Tinea corporis (Fig. 6e) demonstrates moderate clustering, possibly linked to environmental exposure and personal hygiene. Lower-frequency infections such as Tinea unguium (Fig. 6f), Tinea manuum (Fig. 6g), and Tinea pedis (Fig. 6h) show scattered and less dense spatial patterns. However, certain localized pockets still exhibit higher concentrations, indicating specific risk factors such as shared facilities, moisture exposure, or inadequate sanitation. Overall, the spatial analysis indicates that SFI distribution is highly heterogeneous across District Skardu. The presence of distinct hotspots emphasizes the need for targeted public health interventions, including hygiene education, early diagnosis, and localized treatment strategies to effectively control and prevent the spread of fungal infections among School children.
Trend analysis: To reduce the impacts of total trends on the local semi-variant analysis process and more accurately simulate short-range random variation, trend surface analysis was performed in order to obtain SFI trends. Based on the IDW interpolation, the trend analyses of SFI prevalence, incidence and respective. The trend analysis of superficial fungal infections in District Skardu, encompassing overall prevalence, incidence and species-specific trends, is shown in Fig. 7(a-h).
|
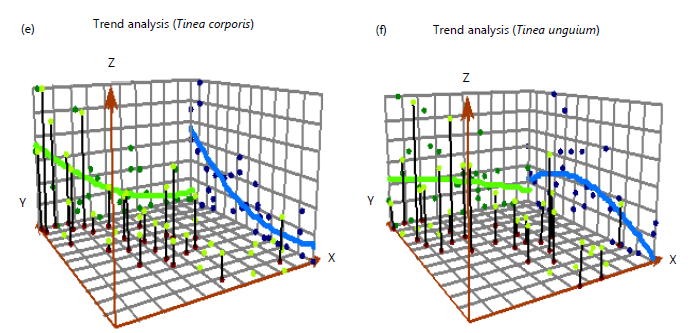
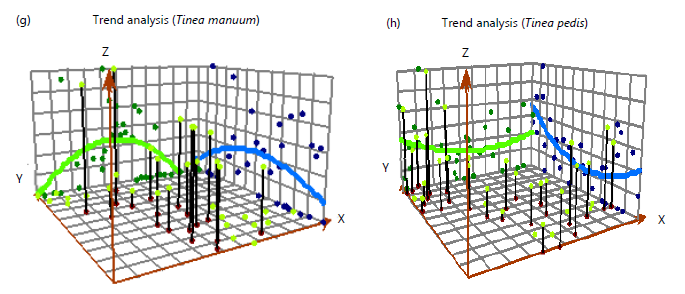
The graphical trends shed light on comparative or temporal shifts in the dynamics of infection. The overall trend of SFI prevalence is shown in Fig. 7a, which shows a generally rising tendency with slight variations over the observed period or groups. These points to a persistent illness burden, which may be impacted by regular exposure to the environment and insufficient protective measures. The trend in disease incidence, which also exhibits variability with sporadic peaks, is shown in Fig. 7b. These peaks might indicate times of higher transmission, which could be related to seasonal variations, school overcrowding, or poor hygiene habits. Significant variations among fungal infections are shown by species-specific patterns (Fig. 7c-h). Tinea capitis (Fig. 7c) shows a fluctuating but slightly increasing trend, indicating its continued dominance among School children, likely due to close contact and sharing of personal items. Tinea faciei (Fig. 7d) exhibits a relatively stable yet moderately increasing pattern, reflecting its widespread nature. Tinea corporis (Fig. 7e) displays variable trends with occasional sharp increases, suggesting episodic outbreaks possibly associated with environmental or behavioural factors. In contrast, Tinea unguium (Fig. 7f) shows a gradual and relatively low trend, indicating limited but persistent occurrence. Similarly, Tinea manuum (Fig. 7g) and Tinea pedis (Fig. 7h) demonstrate low but fluctuating trends, with occasional increases that may be linked to specific risk conditions such as moisture exposure or poor sanitation. Overall, the trend analysis indicates that while some infections remain consistently prevalent, others show variability and episodic increases. This highlights the dynamic nature of SFI transmission in the study area. The observed trends emphasize the importance of continuous monitoring, seasonal preparedness, and implementation of targeted intervention strategies, including hygiene promotion and early treatment, to effectively control the spread of fungal infections among School children.
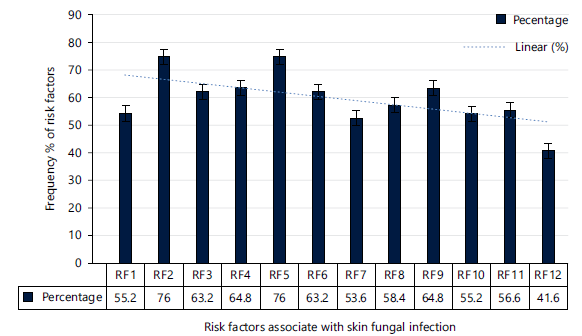
Risk factors for skin fungal infections among study subjects: To assess the twelve dominant risk factors associated with surficial fungal infections, data was collected using a structured questionnaire. The results revealed the following: 55.2% of individuals live in joint family systems, 76.0% have access to pit latrine facilities, 64.8% play with pets, and 76.0% share materials such as combs, head brushes, clothes, and socks.
|
Additionally, 63.2% play games with mud and share towels with family members, while 53.6% frequently have body contact with school mats. Furthermore, 58.4% lack knowledge of personal hygiene, 64.8% live in overcrowded conditions, 55.2% are from low socio-economic backgrounds, and 56.6% have a family history of skin infections. Finally, 41.6% bathe only twice a week (Fig. 8).
DISCUSSION
Understanding the spatial epidemiology, causes, and risk factors of surficial fungal infections (SFIs) is crucial for developing effective prevention strategies and timely interventions. This information is particularly important in school environments, where children are most vulnerable to these infections. SFIs are a significant health concern among School children and primarily affect the outer layers of the skin, hair, face, feet and nails and are caused by a variety of fungal pathogens. In the current study, spatial epidemiology and associated risk factors have been carried out in North parts of Pakistan. The results revealed that the epidemiology of SFI is varied within the valleys even with the schools. During studies it is documented that many risk factor associated with SFI distribution. The distribution SFI among School children varies depending on geographic location, climate, behaviour, knowledge and socioeconomic factors. Many studies have been documented that SFI is most common all over the world especially in developing countries. Kundu et al.14 reported in India 11.6% of School children between the age of 5-14 infected with fungal species T. corporis and T. capitis. Similar studies also conducted in Sub-Saharan Africa and reported high prevalence of SFI in School children and these infection accelerated when environmental condition conducive for fungal growth15. (More or less similar reports are published different research in the different areas of World which is agreement to our studies that School children are more vulnerable groups of SFI.
In developed countries, while the overall prevalence might be lower compared to developing and under developed countries. Havlick et al.15 reported that in the United states approximately 10% SFI in School children with a dominant species is T. pedis. Several influencing factors contribute to the high incidence of SFI can categorized into environmental, behavioral, and individual characteristics. The environmental factor especially warm and humid provides ideal condition for fungal growth and infection in different parts of body. Studies have shown that regions with high temperatures and frequent rainfall exhibit a higher incidence of dermatophyte infections12. Furthermore, overcrowded schools and poor sanitation practices exacerbate the spread of fungi. Shared facilities like locker rooms, bathrooms, and gym showers create an environment where fungal infections can easily spread among children. Physical activities like football, basketball, and swimming creates excessive sweating, which creates an environment conducive to fungal growth16. Additionally, the sharing of personal items like towels, combs, and shoes is a key factor in the transmission of fungal infections and children with compromised immune systems, such as those with diabetes or malnutrition, are more vulnerable to fungal infections13. The statement is agreement with our study that nutritional security situation for children in Skardu is precarious, with high rates of malnutrition driven by food insecurity, limited dietary diversity, and insufficient access to healthcare and nutrition education17. The present study documneted highly special distribution of SFI and respective species in School children of study areas This occurrence relates to that found in earlier studies conducted by other researchers16-18conditions that increase the likelihood of cutaneous fungal infections in the investigated sample. This conclusion also reflects the low socioeconomic level prevalent in the studied area. Many researchers19-23 highlighted similar environmental factors in their study areas, including a low socioeconomic class of populations, lack of personal hygiene among children, a low level of education, insufficient healthy environmental measures, inadequate water availability, and adverse socio-cultural practices. Because skin fungal infections are a disease of poverty, the various communities must take significant action to solve the issue24.
CONCLUSION
The findings demonstrate considerable spatial variation in the prevalence and incidence of superficial fungal infections among School children in Gilgit-Baltistan, with multiple socioeconomic and behavioral factors contributing to disease transmission. Key risk factors include poor hygiene practices, shared personal items, close household contact, and limited sanitation facilities. These results underscore the need for targeted health education and preventive interventions in school settings. Implementing such strategies can reduce disease burden, improve child health outcomes, and support the development of effective public health policies in resource-limited regions.
SIGNIFICANCE STATEMENT
This study provides the first spatial epidemiological evidence of superficial fungal infections among School children in North Pakistan, highlighting substantial geographic variation and key modifiable risk factors. The findings offer important baseline data for identifying high-risk areas and vulnerable populations, supporting targeted public health interventions. By integrating GIS-based analysis with epidemiological data, the study contributes to improved disease surveillance and prevention strategies in school settings, particularly in resource-limited and geographically fragile regions.
FUNDING
This research is funded by the Health Research Institute (HRI), National Institute of Health Islamabad Pakistan under grant no SG-22/R3-59. The authors would like to thank the National Institute of Health (NIH) for fiscal assistance in research.
ACKNOWLEDGMENT
We thank the primary School children in District Skardu North Pakistan who gave consent for this research.
REFERENCES
- Hafeez, A., W.J. Dangel, S.M. Ostroff, A.G. Kiani and S.D. Glenn et al., 2023. The state of health in Pakistan and its provinces and territories, 1990-2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet Global Health, 11: e229-e243.
- Ezomike, N.E., A.N. Ikefuna, C.L. Onyekonwu, A.C. Ubesie, U.R. Ojinmah and B.C. Ibe, 2021. Epidemiology and pattern of superficial fungal infections among primary School children in Enugu, South-East Nigeria. Malawi Med. J., 33: 21-27.
- Bongomin, F., S. Gago, R.O. Oladele and D.W. Denning, 2017. Global and multi-national prevalence of fungal diseases-estimate precision. J. Fungi, 3.
- Nweze, E.I. and I.E. Eke, 2018. Dermatophytes and dermatophytosis in the Eastern and Southern parts of Africa. Med. Mycol., 56: 13-28.
- Longley, P.A., 2015. Analysis Using Geographic Information Systems. In: Handbook of Research Methods and Applications in Economic Geography, Karlsson, C., M. Andersson and T. Norman (Eds.), Edward Elgar Publishing, Cheltenham, United Kingdom, ISBN: 9780857932679, pp: 119-134.
- Enwin, A.D., T.D. Ikiriko and V.K. Peter, 2024. Using geographic information systems as methodologies in architecture and urban planning research. Int. J. Res. Publ. Rev., 5: 4064-4082.
- Oke, O.O., O. Onayemi, O.A. Olasode, A.G. Omisore and O.A. Oninla, 2014. The prevalence and pattern of superficial fungal infections among School children in Ile-Ife, South-Western Nigeria. Dermatol. Res. Pract., 2014.
- Ameen, M., 2010. Epidemiology of superficial fungal infections. Clin. Dermatol., 28: 197-201.
- Hussain, A., S. Ali, H. Abbas, H. Ali, A. Hussain and S.W. Khan, 2019. Spatial distribution of early blight disease on tomato, climatic factors and bioefficacy of plant extracts against Alternaria solani. Acta Sci. Pol. Hortorum Cultus, 18: 29-38.
- Gumprecht, D., W.G. Müller and J.M. Rodríguez-Díaz, 2009. Designs for detecting spatial dependence. Geogr. Anal., 41: 127-143.
- Solouki, A., J.Á. Berna-Sicilia, A. Martinez-Alonso, N. Ortiz-Delvasto, G. Bárzana and M. Carvajal, 2023. Onion plants (Allium cepa L.) react differently to salinity levels according to the regulation of aquaporins. Heliyon, 9.
- Hussain, A., M.S. Awan, S. Ali, S.W. Khan, F. Morari and S. Ali, 2016. Spatial variability of soil micronutrients (Cu, Fe, Zn & Mn) and population dynamic of mycoflora in potato fields of CKNP region Gilgit-Baltistan Pakistan. Pak. J. Agri. Sci., 53: 541-550.
- Bongomin, F., R. Olum, L. Nsenga, M. Namusobya and L. Russell et al., 2021. Estimation of the burden of Tinea capitis among children in Africa. Mycoses, 64: 349-363.
- Kundu, D., L. Mandal and G. Sen, 2012. Prevalence of Tinea capitis in school going children in Kolkata, West Bengal. J. Nat. Sci. Biol. Med., 3: 152-155.
- Ortiz, B., F. Morio, K. Aguilar, F. García, G. Fontecha and A. Moreno-Sabater, 2026. T. indotineae: A new emergent fungal pathogen driven by global travel. Mycoses, 69.
- Adefemi, S.A., L.O. Odeigah and K.M. Alabi, 2011. Prevalence of dermatophytosis among primary School children in Oke-Oyi community of Kwara State. Niger. J. Clin. Pract., 14: 23-28.
- Seebacher, C., J.P. Bouchara and B. Mignon, 2008. Updates on the epidemiology of dermatophyte infections. Mycopathologia, 166: 335-352.
- Reichert-Pénétrat, S., N. Contet-Audonneau, A. Barbaud, J.P. Schurra, B. Fortier and J.L. Schmutz, 2002. Epidemiology of dermatophytoses in children living in Northeast France: A 5-year study. Pediatr. Dermatol., 19: 103-105.
- Bongomin, F. and S.A. Fayemiwo, 2021. Epidemiology of fungal diseases in Africa: A review of diagnostic drivers. Curr. Med. Mycol., 7: 63-70.
- Pires, C.A.A., N.F.S. da Cruz, A.M. Lobato, P.O. de Sousa, F.R.O. Carneiro and A.M.D. Mendes, 2014. Clinical, epidemiological, and therapeutic profile of dermatophytosis. Anais Brasileiros Dermatologia, 89: 259-264.
- Balci, E., M. Gulgun, O. Babacan, A. Karaoglu and V. Kesik et al., 2014. Prevalence and risk factors of tinea capitis and tinea pedis in School children in Turkey. J. Pak. Med. Assoc., 64: 514-518.
- İnanir, I., M.T. Şahin, K. Gündüz, G. Dinç, A. Türel and S. Öztürkcan, 2002. Prevalence of skin conditions in primary School children in Turkey: Differences based on socioeconomic factors. Pediatr. Dermatol., 19: 307-311.
- Figueroa, J.L., L.C. Fuller, A. Abraha and R.J. Hay, 1996. The prevalence of skin disease among School children in rural Ethiopia-a preliminary assessment of dermatologic needs. Pediatr. Dermatol., 13: 378-381.
- Havlickova, B., V.A. Czaika and M. Friedrich, 2008. Epidemiological trends in skin mycoses worldwide. Mycoses, 51: 2-15.
How to Cite this paper?
APA-7 Style
Hussain,
A., Nafees,
M.A., Abbas,
G., Din,
S.u. (2026). Spatial Epidemiology and Risk Factors Associated with Surficial Fungal Infection in Schoolchildren of North Pakistan. Trends in Biological Sciences, 2(3), 265-279. https://doi.org/10.21124/tbs.2026.265.279
ACS Style
Hussain,
A.; Nafees,
M.A.; Abbas,
G.; Din,
S.u. Spatial Epidemiology and Risk Factors Associated with Surficial Fungal Infection in Schoolchildren of North Pakistan. Trends Biol. Sci 2026, 2, 265-279. https://doi.org/10.21124/tbs.2026.265.279
AMA Style
Hussain
A, Nafees
MA, Abbas
G, Din
Su. Spatial Epidemiology and Risk Factors Associated with Surficial Fungal Infection in Schoolchildren of North Pakistan. Trends in Biological Sciences. 2026; 2(3): 265-279. https://doi.org/10.21124/tbs.2026.265.279
Chicago/Turabian Style
Hussain, Azhar, Maisoor Ahmad Nafees, Ghulam Abbas, and Saif ud Din.
2026. "Spatial Epidemiology and Risk Factors Associated with Surficial Fungal Infection in Schoolchildren of North Pakistan" Trends in Biological Sciences 2, no. 3: 265-279. https://doi.org/10.21124/tbs.2026.265.279

This work is licensed under a Creative Commons Attribution 4.0 International License.