Thrombin Time Clotting Assay as a Predictor Marker of Bleeding Risk in Individuals with Non-Alcoholic Fatty Liver Disease in Calabar, Nigeria
-
Mbang Kooffreh-Ada
Department of Internal Medicine, University of Calabar Teaching Hospital, Calabar, Nigeria
Dorathy Chioma Okpokam

Department of Haematology and Blood Transfusion Science, University of Calabar, Calabar, Nigeria
Kitu David EmengDepartment of Haematology and Blood Transfusion Science, University of Calabar, Calabar, Nigeria
Gift Thomas EtengDepartment of Haematology and Blood Transfusion Science, University of Calabar, Calabar, Nigeria
Nkeiruka Ogo OgidiDepartment of Medical Laboratory Science, University of Lagos, Lagos, Nigeria
Chukwuka Onyedikachim OparaDepartment of Haematology and Blood Transfusion Science, University of Calabar, Calabar, Nigeria
Ehijie Xavier IyamahUniversity of Benin Teaching Hospital, Benin, Nigeria
Ogha Eyamnzie OkpokamEpidemiology and Public Health, Achieving Health Nigeria Initiative, Nnewi, Nigeria
| Received 07 Oct, 2025 |
Accepted 20 Dec, 2025 |
Published 31 Dec, 2025 |
Background and Objective: Non-Alcoholic Fatty Liver Disease (NAFLD) has become the leading cause of liver disease, and its prevalence is projected to rise further as obesity rates increase and the global population continues to age. This study aims to investigate the coagulation parameters in individuals with Non-Alcoholic Fatty Liver Disease (NAFLD) attending the clinic at Medicine Outpatient and Internal Medicine Department, University of Calabar Teaching Hospital, Calabar, Nigeria. Methods and Methods: A case study design was used in the study at Medicine Outpatient, Family Medicine of the University of Calabar Teaching Hospital, Calabar. A total of 40 subjects (20 controls and 20 patients) were selected. Citrate samples were used, and PT, APTT, and TT testing were performed using the Quick One-Stage method. The results were presented in percentages, student’s t-test, and Pearson’s correlation, p<0.05. Results: The demographic distribution with the highest percentage age range of 40-60 (70%), male (45%), female (55%), married individuals (100%), and duration of having NAFLD 2 years and above (95%). The NAFLD patients had higher mean values of BMI, SBP, and DBP vital signs (36 kg/m2, 138 and 85 mmHg) than the control subjects (26 kg/m2, 106 mmHg, and 68 mmHg). The TT parameters show a strongly significant (p<0.05) prolongation in NAFLD patients (21 sec) when compared with the control subjects (13 sec), while APTT shows mild prolongation. Females had a higher value of weight in contrast to males. There was also a mild positive correlation (r = 0.212; p<0.05) between TT and APTT of NAFLD patients. Conclusion: The finding of this study suggests that TT should be included as a marker for easy investigation of NAFLD and to identify potential bleeding or clotting risks for proper management.
| Copyright © 2025 Kooffreh-Ada et al. This is an open-access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. |
INTRODUCTION
Non-Alcoholic Fatty Liver Disease (NAFLD) is characterized by the accumulation of fat in more than 5% of hepatocytes, occurring due to insulin resistance and in the absence of secondary causes of liver steatosis1. It represents a spectrum of histological alterations, ranging from Non-Alcoholic Fatty Liver (NAFL) or simple steatosis to Non-Alcoholic Steatohepatitis (NASH), characterized by hepatocellular injury, degeneration, and progressive fibrosis that may progress to cirrhosis and hepatocellular carcinoma2-5.
The NAFLD is not related to excessive alcohol consumption but is strongly associated with metabolic syndrome components such as obesity, diabetes, high cholesterol, and cardiovascular diseases6. Recent studies have indicated that NAFLD patients may exhibit alterations in the coagulation system, leading to an increased risk of developing clotting disorders. The most common coagulation dysfunctions observed include clotting factor deficiencies, hypercoagulable states, and deep-venous thrombosis. These dysfunctions occur during NAFLD progression due to the liver’s impaired ability to secrete coagulation factors7-9.
Understanding the impact of NAFLD on coagulation parameters is essential for evaluating the overall hemostatic balance in patients, identifying potential bleeding risks, predicting disease progression, and informing treatment decisions. Research has revealed that NAFLD is associated with a relatively hypercoagulable state, although the precise underlying mechanisms remain unknown10-12. Additionally, studies have shown that NAFLD is characterized by marked hypofibrinolysis, especially in patients with steatohepatitis, who exhibit high levels of Plasminogen Activator Inhibitor-1 (PAI-1) and prolonged clot lysis times13,14. These findings underscore the importance of monitoring coagulation parameters in NAFLD patients to manage and mitigate potential complications effectively. The purpose of this study is therefore to investigate the haemostatic profile of individuals with NAFLD, to identify early coagulation abnormalities that may predispose them to thrombotic or bleeding risks. By understanding these alterations, the study aims to contribute to improved clinical assessment, risk stratification, and patient management.
MATERIALS AND METHODS
Study design: This case-control study comprised a total of forty subjects, grouped into twenty fatty liver disease patients and twenty apparently healthy control subjects. Sample size calculation was done15 using a prevalence of 4.5%16.
Study area and population: The test subjects were recruited from the Medicine Outpatient, Family Medicine, and Internal Medicine Departments of the University of Calabar Teaching Hospital (UCTH), Calabar.
Ethical approval and informed consent: Ethical approval was obtained from the Health Research Ethical Committee (HREC) of the University of Calabar Teaching Hospital, Calabar, with Registration Number: NHREC/07/10/2012 and Approval Number: UCTH/HREC/33/Vol.III/151. Written informed consent was also obtained from all participants before enrollment.
Data collection and parameters assessed: Anthropometric variables, fasting blood glucose, triglyceride, total and High-Density Lipoprotein Cholesterol (HDL-C), and blood pressure were assessed using a structured questionnaire with assistance from clinicians.
Duration of study: The study was conducted over a period of seven months, from June to December, 2023, following ethical clearance and participant consent.
Inclusion criteria: Subjects were included in the study if they met the following conditions:
| • | Diagnosis of NAFLD: Confirmed by ultrasound, liver biopsy, along with elevated liver enzymes (ALT/AST) and/or imaging findings consistent with hepatic steatosis | |
| • | No history of significant alcohol intake (≤20 g/day for women, ≤30 g/day for men) or other known causes of liver disease (e.g., viral hepatitis, autoimmune liver diseases, drug-induced liver injury) | |
| • | Presence of one or more metabolic risk factors such as obesity (BMI ≥25 kg/m2), type 2 diabetes mellitus, dyslipidemia, or hypertension | |
| • | Control group screening: Control subjects were screened using liver ultrasound and liver function tests (ALT and AST) to rule out fatty liver disease | |
| • | Age criteria: Adults aged 18-70 years were included | |
| • | Willingness to participate: Subjects provided informed consent and agreed to complete necessary laboratory tests and assessments |
Exclusion criteria: Subjects were excluded from the study if they met any of the following conditions:
| • | No NAFLD diagnosis: Individuals who did not have NAFLD based on imaging and biochemical assessments | |
| • | Presence of hepatitis B or C, autoimmune hepatitis | |
| • | Excessive alcohol consumption: Alcohol intake exceeding 20 g/day for women and 30 g/day for men | |
| • | Subjects with chronic kidney disease, active malignancy, severe cardiovascular disease, HIV, or other systemic inflammatory conditions | |
| • | Women who were pregnant or breastfeeding | |
| • | Unwillingness to participate: Subjects who declined to provide informed consent or were unable to comply with study procedures |
Sample collection and testing: As 4.5 mL of blood were collected from all subjects and delivered into 0.5 mL of 3.13 trisodium citrate anticoagulant. It was mixed and centrifuged at 1500 g for 15 min to obtain the platelet poor plasma (PPP). It was frozen at -20°C until ready to analyze. The citrated sample was then analyzed with Prothrombin time test, activated partial prothrombin time, and Thrombin time test reagents (Helena Bioscience) using the One Stage Quick clot-based Method by Dacie and Lewis Practical Haematology17, and according to the manufacturer’s instructions.
The prothrombin time (PT) test was carried out by adding tissue thromboplastin and calcium chloride to platelet-poor plasma to determine the clotting time at 37°C. Khan tubes labelled as test and control were pre-warmed, after which 0.1 mL of plasma was introduced into each tube and allowed to warm for one minute. Tissue thromboplastin and calcium were then added, and the stopwatch was started immediately. The tubes were gently tilted at intervals until clot formation was observed. The procedure was repeated in duplicates, and the average value was recorded. The reference range for PT was 10-14 sec.
The Activated Partial Thromboplastin Time (APTT) test, also referred to as PTTK, was performed to assess the intrinsic and common coagulation pathways. Clean glass tubes of uniform diameter were pre-warmed at 37°C before 0.1 mL of platelet-poor plasma was added. A commercially prepared PTTK reagent was added and incubated for 3 min. Calcium chloride was then introduced, and the stopwatch was started immediately. The tubes were tilted once per second to observe clot formation, and the clotting time was recorded. Both test and control samples were analysed in duplicates, and the mean time was documented. The reference range for APTT was 30-40 sec.
The thrombin time (TT) test was performed by adding thrombin to plasma to measure the conversion of fibrinogen to fibrin. Pre-warmed glass tubes received 0.1 mL of thrombin solution, followed by 0.2 mL of control plasma, and the stopwatch was started as the reaction began. The clotting time and the physical characteristics of the clot-such as transparency or firmness-were noted. The same procedure was repeated with patient plasma samples in duplicate and with an additional control sample. The reference range for TT was 15-19 sec.
Statistical analysis: Data was presented in tables and graphs as standard deviation (SD). The Statistical Package for the Social Sciences (SPSS) 23 was used in the analysis of the results. Comparison was made between the two groups using the Student’s t-test. Pearson correlation was also used to determine relationships. The p-value at ≤0.05 was considered statistically significant.
RESULTS
The study was to investigate some coagulation profiles, such as prothrombin time (PT), Activated Partial Thromboplastin Time (APTT), and thrombin time (TT), in individuals with non-alcoholic fatty liver disease attending the clinic in the University of Calabar Teaching Hospital, Calabar, Nigeria. The following vital parameters were carried out: Age, weight, height, waist, hip, Body Mass Index (BMI), systolic blood pressure (SBP), diastolic blood pressure (DBP), and abdominal scan. Table 1 shows the demographic distribution of control and non-alcoholic fatty liver disease patients. The age range of both control and non-alcoholic fatty liver disease patients was between 20 and 80, and they comprise 3 groups, which are 20-39, 40-60 years, and 61-80 years. It was observed that the non-alcoholic fatty liver disease patients age group of 40-60 years (70%) had the highest percentage, followed by 61-80 years (30%). In the gender, the female had the highest percentage (55%) while the male had (45%).
| Table 1: | Demographic profile of Non-Alcoholic Fatty Liver Disease (NAFLD) and control subjects | |||
| Demographics | NAFLD subjects | Control subjects |
| n = 20 | n = 20 | |
| N (%) | N (%) | |
| Age range (years) | ||
| 20-39 | 0 | 13 (65%) |
| 40-60 | 14 (70%) | 7 (35%) |
| 61-80 | 6 (30%) | 0 |
| Gender | ||
| Male | 9 (45%) | 10 (50%) |
| Female | 11 (55%) | 10 (50%) |
| Marital status | ||
| Married | 20 (100%) | 10 (50%) |
| Single | 10 (50%) | |
| Occupation | ||
| Student | 0 | 5 (25%) |
| Business trader | 7 (35%) | 2 (10%) |
| Self-employed | 0 | 4 (20%) |
| Health worker | 1 (5%) | 4 (20%) |
| Civil servant | 11 (55%) | 5 (25%) |
| Retired | 1 (5%) | 0 |
| Lifestyle factors | ||
| Exercise | ||
| Yes | 3 (15%) | 14 (70%) |
| No | 17 (85%) | 6 (30%) |
| Junk consumers | ||
| Yes | 12 (60%) | 4 (20%) |
| No | 8 (40%) | 16 (80%) |
| Alcohol consumers | ||
| Yes | 5 (25%) | 2 (10%) |
| No | 15 (75%) | 18 (90%) |
| Duration | ||
| 7 months-1 year | 1 (5%) | 0 |
| 2 years and above | 19 (95%) | |
| NAFLD: Non-alcoholic fatty liver disease, n: Number of subjects enrolled, N: Frequency | ||
| Table 2: | Vital signs and some coagulation parameters of non-alcoholic fatty liver disease patients and control subjects | |||
| Parameter | NAFLD subjects (n = 20) | Control | p-value |
| Age (years) | 58.1±8.79 | 34.4±12.1 | 0.057 |
| Weight (kg) | 98.4±5.9 | 72.6±10.4 | 0.08 |
| Height (m) | 1.7±0.1 | 1.7±0.1 | 0.64 |
| BMI (kg/m2) | 35.8±4.5 | 26.3±2.6 | 0.009* |
| Waist (in) | 43.6±4.0 | 35.2±4.0 | 0.959 |
| Hip (in) | 46.3±4.97 | 40.5±3.7 | 0.055 |
| SBP (mmHg) | 137.8±11.9 | 108.5±14.4 | 0.025* |
| DBP (mmHg) | 84.8±4.99 | 68.1±6.95 | 0.033* |
| PT (sec) | 15.9±3.1 | 12.3±1.9 | 0.076 |
| APTT (sec) | 32.8±6.8 | 32.1±3.96 | 0.035* |
| TT (sec) | 21.0±10.6 | 13.4±1.5 | 0.001* |
| BMI: Body mass index, SBP: Systolic blood pressure, DBP: Diastolic blood pressure, PT: Prothrombin time, APTT: Activated partial thromboplastin time, TT: Thrombin time, Kg: Kilograms, m: Meters, kg/m2: Kilograms per meters square, in: Inches, mmHg: Millimeters of mercury, Sec: Seconds and *Significant at p<0.05 | |||
| Table 3: | Vital signs and some coagulation parameters of non-alcoholic fatty liver disease patients based on age | |||
| Parameter | 40-60 years (n = 14) | 61-80 years (n = 6) | p-value |
| Weight (kg) | 98.7±6.97 | 97.5±2.4 | 0.010* |
| Height (m) | 1.7±1.1 | 1.7±0.1 | 0.029* |
| BMI (kg/m2) | 36.7±4.99 | 33.9±2.6 | 0.047* |
| Waist (in) | 43.4±4.5 | 44.0±3.0 | 0.338 |
| Hip (in) | 47.2±5.2 | 44.0±4.1 | 0.394 |
| SBP (mmHg) | 139.3±10.2 | 134.2±15.6 | 0.164 |
| DBP (mmHg) | 85.6±5.3 | 83.0±3.9 | 0.611 |
| Abdominal scan (cm) | 15.9±0.96 | 15.5±0.89 | 0.724 |
| PT (sec) | 15.9±3.1 | 15.8±3.4 | 0.556 |
| APTT (sec) | 33.4±7.4 | 31.3±5.6 | 0.44 |
| TT (sec) | 21.1±10.2 | 20.8±12.6 | 0.616 |
| BMI: Body mass index, SBP: Systolic blood pressure, DBP: Diastolic blood pressure, PT: Prothrombin time, APTT: Activated partial thromboplastin time, TT: Thrombin time, Kg: Kilograms, m: Meters, kg/m2: Kilograms per meters square, in: Inches, mmHg: Millimeters of mercury, cm: Centimeters, sec: Seconds and *Significant at p<0.05 | |||
The marital status shows that the married group had the highest percentage. Their occupation shows that civil servants had the highest percentage (55%), followed by business traders (35%), then health workers and retirees having the smallest percentage (5%), respectively. The lifestyle factors data show that a higher percentage of the patients do not exercise (85%), while a smaller percentage (15%) do. Sixty percent are junk consumers (pastry), 40% are not, but occasionally eat outside. A smaller percentage of the subjects (25%) consume alcohol in small amounts, and a greater percentage (75%) do not consume alcohol, indicating that the disease is not alcohol dependent. The duration was in two groups: 7 months to 1 year, and 2 years and above. The group of 2 years and above had a greater percentage (95%), while 7 months to 1 year had a lesser percentage (5%). Table 2 shows the comparison between vital signs and some coagulation parameters of Non-Alcoholic Fatty Liver Disease Patients (NAFLD) and the control group (without fatty liver disease) of the study.
The mean values of the parameters (age, weight, height, BMI, waist, hip, SBP, DBP and abdominal scan) for the NAFLD are 58.1 years, 98.4 kg, 1.7 m, 35.8 kg/m2, 43.6 in, 46.3 in, 137.8 mmHg, 84.8 mmHg, and 15.8 cm and control are 34.4 years, 72.6 kg, 1.7 m, 26.3 kg/m2, 35.2 in, 40.5 in, 108.5 mmHg and 68.1 mmHg. There was a significant (p<0.05) increase in the BMI of NAFLD when compared with the control subjects. Meanwhile, the mean values of the coagulation parameters (APTT and TT) of NAFLD were 32.8 and 21.0 sec, and were found to be statistically prolonged (p<0.001) when compared with the control group, 32.1 and 13.4 sec. There was no significant difference in PT value when the two groups were compared.
|
| Table 4: | Vital signs and some coagulation parameters of non-alcoholic fatty liver disease patients based on gender | |||
| Parameter | Male (n = 9) | Female (n = 11) | p-value |
| Weight (kg) | 97.3±2.7 | 99.2±7.7 | 0.002* |
| Height (m) | 1.7±0.1 | 1.6±0.1 | 0.71 |
| BMI (kg/m2) | 32.5±2.7 | 38.5±3.9 | 0.063 |
| Waist (in) | 43.2±3.2 | 43.9±4.7 | 0.252 |
| Hip (in) | 42.2±3.1 | 49.6±3.6 | 0.583 |
| SBP (mmHg) | 132.8±12.5 | 141.8±10.1 | 0.632 |
| DBP (mmHg) | 83.6±3.3 | 85.8±6.0 | 0.099 |
| Abdominal scan (cm) | 15.8±0.9 | 15.8±0.99 | 0.726 |
| PT (sec) | 15.4±3.6 | 16.3±2.7 | 0.588 |
| APTT (sec) | 32.8±8.3 | 32.8±5.7 | 0.121 |
| TT (sec) | 19.8±9.4 | 22.0±11.8 | 0.238 |
| BMI: Body mass index, SBP: Systolic blood pressure, DBP: Diastolic blood pressure, PT: Prothrombin time, APTT: Activated partial thromboplastin time, TT: Thrombin time, kg: kilograms, m: Meters, kg/m2: Kilograms per meters square, in: Inches, mmHg: Millimeters of mercury, cm: Centimeters, Sec: Seconds and *Significant at p<0.05 | |||
Table 3 shows the comparison of the vital signs and coagulation parameters of non-alcoholic fatty liver disease patients based on age. Out of 20 subjects enrolled in the study, the table shows mean value of subjects from age range 40-60 years with the parameters (weight, height, body mass index, waist, hip, systolic blood pressure, diastolic blood pressure and abdominal scan) are 98.7 kg, 1.7 m, 36.7 kg/m2, 43.4 in, 47.2 in, 139.3 mmHg, 85.6 mmHg and 15.9 cm. The mean values of the age range 61-80 years are 97.5 kg, 1.7 m, 33.9 kg/m2, 44.0 in, 44.0 in, 134.2 mmHg, 83.0 mmHg, and 15.5 cm. There was a statistically significant increase (p<0.05) in the mean values of weight, height, and BMI in the age range 40-60 years when compared to 61-80 years. Meanwhile, in the coagulation parameters of (PT, APTT, and TT) the mean values of subjects for the age range 40-60 years are 15.9, 33.4 and 21.1 sec, and 61-80 years are 15.8, 31.3 and 20.8 sec. There was no statistical difference (p>0.05) in the coagulation parameter.
Table 4 shows a comparison of vital signs of non-alcoholic fatty liver disease patients based on gender. The mean value of the vital signs (weight, height, BMI, waist, hip, SBP, DBP and abdominal scan) are 97.3 kg, 1.7 m, 32.5 kg/m2, 43.2 in, 42.2 in, 132.8 mmHg, 83.6 mmHg and 15.8 cm for male, and 99.2 kg, 1.6 m, 38.5 kg/m2, 43.9 in, 49.6 in, 141.8 mmHg, 85.8 mmHg and 15.8 cm for female.
|
|
There was a statistically significant decrease (p<0.05) in the weight of male when compared to females. Meanwhile, mean values of the male subjects with respect to the coagulation parameters (PT, APTT and TT) are 15.4, 32.8 and 19.8 sec, while that of the female subjects are 16.3, 32.8 and 22.0 sec. There was no statistical significance.
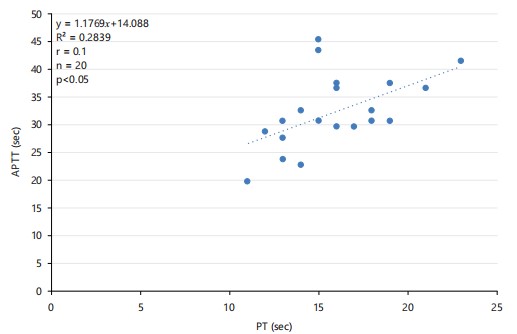
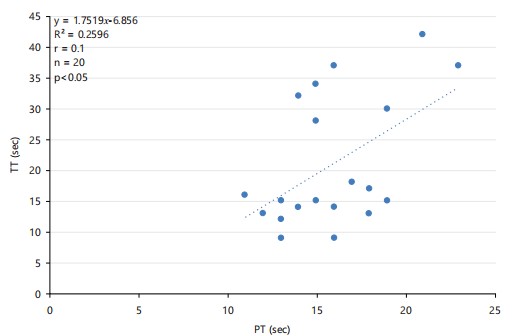
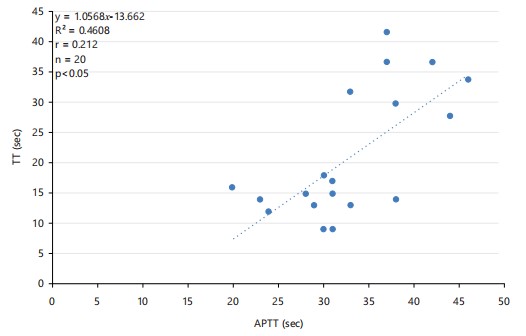
Figure 1 shows the correlation between APTT and PT of patients with Non-Alcoholic Fatty Liver Disease (NAFLD), which was a mild positive correlation. The positive correlation indicates that as APTT increases, PT increases (r = 0.1) (p<0.05). In the correlation between APTT and TT (Fig. 2), patients with NAFLD show a mild positive correlation (r = 0.1) (p<0.05), indicating that as APTT increases, TT increases. Figure 3 shows the correlation between TT and PT of patients with NAFLD. It shows a mildly significant positive correlation (r = 0.2) (p<0.05), which indicates that as TT increases, PT increases.
DISCUSSION
This study assessed prothrombin time (PT), Activated Partial Thromboplastin Time (APTT), and thrombin time (TT) in individuals with Non-Alcoholic Fatty Liver Disease (NAFLD) attending the clinic in the University of Calabar Teaching Hospital (UCTH). Among the 20 Non-Alcoholic Fatty Liver Disease (NAFLD) patients enrolled in this study, it was observed from the socio-demographic parameters captured in Table 1 that the majority of Non-Alcoholic Fatty Liver Disease (NAFLD) patients were in the age bracket of 40-60 years (70%). This could be attributed to their plummeting fitness level due to decreased physical activity, as they tend to favor light activities such as gardening rather than cardio-boosting exercises such as running. In contrast, their peers without NAFLD had steadier fitness levels over the years. This is consistent with the earlier findings that NAFLD is of an increasing prevalence with age18,19.
It also revealed that 55% of the NAFLD patients were females, while males constituted only 45%. The study suggests that it could be a result of the females having a higher Body Mass Index (BMI). This finding agrees with a report that there is increased NAFLD prevalence in women in the transitional post-menopausal stage than male18. In women, elevated BMI, low HDL cholesterol, increased waist and hip circumference, and hyperglycemia were significantly larger contributors to NAFLD, while in men, these were hypertension and elevated triglycerides. When grouped into marital status, it was found that married people were more affected. In this study, this could be as a result of married people consuming junk or occasionally eating unhealthily outside. They could be lacking quality marital life, alongside facing stress at home, which could lead to HBP (High Blood Pressure). This finding is in line with the narrative that married people who have financial problems and household expenses have less interest in engaging in healthy behaviours, including appropriate nutrition and regular exercise. They may not eat an appropriate breakfast or eat other meals at an appropriate time20,21. In this study, it was also observed that the majority of NAFLD patients were civil servants (55%) followed by business traders (35%). This could be attributed to the sedimentary lifestyle associated with their job; civil servants often have desk jobs that involve prolonged hours of sitting, while business traders may also have a predominant work routine. It could also be caused by the unhealthy diet since some civil servants and business traders have limited access to healthy food options. The demands of civil service jobs or the challenges faced by business traders may also lead to increased stress levels, which can contribute to metabolic disturbances and potentially increase the risk of NAFLD. When grouped into duration of 7 months to 1 year, 2 years and above. As 95% of the subjects fell under the 2 years and above bracket; this could be due to the alarming increase in unhealthy lifestyles leading to the development of non-alcoholic fatty liver disease.
It also revealed that the NAFLD subjects had higher values of the coagulation parameters (APTT and TT). This could be owing to various factors, such as liver function affected by inflammation or fibrosis, leading to impaired production of clotting factors and potentially prolonging APTT. This liver dysfunction could disrupt vitamin K metabolism as well as affect the clotting cascade and prolong APTT. It may also affect fibrinogen synthesis, which influences thrombin time, potentially prolonging it. Furthermore, inflammation associated with NAFLD might impact the coagulation system; chronic inflammation can lead to an imbalance in pro-and anti-coagulant factors, affecting APTT and TT. This finding therefore agrees with the report that dysregulation of the coagulation cascade is common in chronic diseases of the liver, such as NAFLD22. Since the liver produces most factors associated with coagulation and fibrinolysis pathways, advanced liver disease of any etiology commonly exhibits disruptions in the coagulation pathway. The NAFLD is associated with a relatively hypercoagulable state. Although the precise underlying mechanisms remain unknown, chronic liver inflammation is likely to be the most important trigger for disrupting the balance of the coagulation system11,23. Research question 1, which required if there is any significant difference in the coagulation profile of patients with non-alcoholic fatty liver disease and control subjects, is therefore positively answered. In line with the findings of this study, it is recommended that the hospital management consider incorporating coagulation parameter assessments as adjunct tests alongside routine investigations. This approach would enable a more comprehensive evaluation of the coagulation profile in patients with Non-Alcoholic Fatty Liver Disease (NAFLD), allowing for better interpretation of potential hemostatic changes. Additionally, there should be enhanced collaboration between clinicians and healthcare workers involved in the management of NAFLD patients to raise awareness about the importance of monitoring variations in coagulation parameters. Early detection of such changes will aid in improving patient management and identifying early markers associated with the progression of coagulation abnormalities in the context of NAFLD. Furthermore, healthcare providers should intensify sensitization programs to educate the public on the existence and risks of NAFLD, emphasizing the role of lifestyle modification, such as maintaining a healthy diet and engaging in regular physical activity, to reduce risk factors like obesity and diabetes.
CONCLUSION
The present study has revealed that NAFLD is more likely to affect women more than men, particularly in particular among the post-menopausal period, and can lead to a significant increase in coagulation parameters, APTT, and TT. There appears to be a mild positive correlation between APTT and PT, TT and PT, TT and APTT. This may suggest potential alterations in the coagulation profile of these patients. The NAFLD is associated with liver dysfunction and changes in clotting factors can occur due to liver involvement. A mild positive correlation indicates that as one of these clotting factors increases, the other also tends to increase, suggesting an interplay between components of the coagulation cascade in NAFLD.
SIGNIFICANCE STATEMENT
This study discovered the significant prolongation of thrombin time (TT) in patients with Non-Alcoholic Fatty Liver Disease (NAFLD), highlighting its potential usefulness as an early and sensitive marker of coagulation imbalance in this population. The identification of TT abnormalities can be beneficial for improving clinical evaluation, guiding timely interventions, and preventing potential bleeding or clotting complications among individuals with NAFLD. By providing evidence of the relationship between TT, APTT, and key clinical parameters, this study enhances understanding of the subtle coagulation changes associated with NAFLD progression. This study will help researchers to uncover the critical areas of coagulation-related alterations in NAFLD that many researchers were not able to explore. Thus, a new theory on NAFLD-associated haemostatic dysfunction may be arrived at.
REFERENCES
- Younossi, Z.M., P. Golabi, J.M. Paik, A. Henry, C. van Dongen and L. Henry, 2023. The global epidemiology of nonalcoholic fatty liver disease (NAFLD) and nonalcoholic steatohepatitis (NASH): A systematic review. Hepatology, 77: 1335-1347.
- Guo, X., X. Yin, Z. Liu and J. Wang, 2022. Non-alcoholic fatty liver disease (NAFLD) pathogenesis and natural products for prevention and treatment. Int. J. Mol. Sci., 23.
- Leoni, S., F. Tovoli, L. Napoli, I. Serio, S. Ferri and L. Bolondi, 2018. Current guidelines for the management of non-alcoholic fatty liver disease: A systematic review with comparative analysis. World J. Gastroenterol., 24: 3361-3373.
- Bessone, F., M.V. Razori and M.G. Roma, 2019. Molecular pathways of nonalcoholic fatty liver disease development and progression. Cell. Mol. Life Sci., 76: 99-128.
- Machado, M.V. and A.M. Diehl, 2016. Pathogenesis of nonalcoholic steatohepatitis. Gastroenterology, 150: 1769-1777.
- Caturano, A., C. Acierno, R. Nevola, P.C. Pafundi and R. Galiero et al., 2021. Non-alcoholic fatty liver disease: From pathogenesis to clinical impact. Processes, 9.
- Robea, M.A., I.M. Balmus, I. Girleanu, L. Huiban and C. Muzica et al., 2023. Coagulation dysfunctions in non-alcoholic fatty liver disease-oxidative stress and inflammation relevance. Medicina, 59.
- Pant, A., A.K. Kopec and J.P. Luyendyk, 2018. Role of the blood coagulation cascade in hepatic fibrosis. Am. J. Physiol. Gastrointest. Liver Physiol., 315: G171-G176.
- Premkumar, M. and S.K. Sarin, 2020. Current concepts in coagulation profile in cirrhosis and acute‐on‐chronic liver failure. Clin. Liver Dis., 16: 158-167.
- Kim, C.Y., N. Kim and J.H. Roh, 2023. Association of nonalcoholic fatty liver disease and venous thromboembolic disease in healthy adults in Korea: A nationwide study. Sci. Rep., 13.
- Ciavarella, A., D. Gnocchi, C. Custodero, G.M. Lenato, G. Fiore, C. Sabbà and A. Mazzocca, 2021. Translational insight into prothrombotic state and hypercoagulation in nonalcoholic fatty liver disease. Thromb. Res., 198: 139-150.
- Stine, J.G., B.A. Niccum, A.N. Zimmet, N. Intagliata, S.H. Caldwell, C.K. Argo and P.G. Northup, 2018. Increased risk of venous thromboembolism in hospitalized patients with cirrhosis due to non-alcoholic steatohepatitis. Clin. Transl. Gastroenterol., 9.
- Eriksen, P.L., K.L. Thomsen, M. Sørensen, H. Vilstrup and A.M. Hvas, 2022. Impaired fibrinolysis without hypercoagulability characterises patients with non-alcoholic fatty liver disease. Thromb. Res., 213: 9-15.
- Tripodi, A., A.L. Fracanzani, M. Primignani, V. Chantarangkul and M. Clerici et al., 2014. Procoagulant imbalance in patients with non-alcoholic fatty liver disease. J. Hepatol., 61: 148-154.
- Das, S., K. Mitra and M. Mandal, 2016. Sample size calculation: Basic principles. Indian J. Anaesth., 60: 652-656.
- Onyekwere, C.A., A.O. Ogbera and B.O. Balogun, 2011. Non-alcoholic fatty liver disease and the metabolic syndrome in an urban hospital serving an African community. Ann. Hepatol., 10: 119-124.
- Bain, B.J., S.M. Lewis and J.V. Dacie, 2012. Dacie and Lewis Practical Haematology. 12th Edn., Elsevier, Amsterdam, Netherlands, ISBN-13: 9780702069253, Pages: 600.
- Younossi, Z.M., A.B. Koenig, D. Abdelatif, Y. Fazel, L. Henry and M. Wymer, 2016. Global epidemiology of nonalcoholic fatty liver disease-meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology, 64: 73-84.
- Motamed, N., M. Maadi, M. Sohrabi, H. Keyvani, H. Poustchi and F. Zamani, 2016. Rural residency has a protective effect and marriage is a risk factor for NAFLD. Hepatitis Mon., 16.
- Fu, R. and H. Noguchi, 2016. Does marriage make us healthier? Inter-country comparative evidence from China, Japan, and Korea. PLoS ONE, 11.
- Okpokam, D.C., D.L. Muoka, M. Kooffreh-Ada, I. Isong, O.E. Okpokam and H.A. Efobi, 2024. Evaluation of different diagnostic strategies in the assessment and management of metabolic syndrome patients in South, Nigeria. Asian Sci. Bull., 2: 304-315.
- Northup, P.G. and S.H. Caldwell, 2013. Coagulation in liver disease: A guide for the clinician. Clin. Gastroenterol. Hepatol., 11: 1064-1074.
- Chen, J. and D.W. Chung, 2018. Inflammation, von Willebrand factor, and ADAMTS13. Blood, 132: 141-147.
How to Cite this paper?
APA-7 Style
Kooffreh-Ada,
M., Okpokam,
D.C., Emeng,
K.D., Eteng,
G.T., Ogidi,
N.O., Opara,
C.O., Iyamah,
E.X., Okpokam,
O.E. (2025). Thrombin Time Clotting Assay as a Predictor Marker of Bleeding Risk in Individuals with Non-Alcoholic Fatty Liver Disease in Calabar, Nigeria. Trends in Biological Sciences, 1(4), 306-315. https://doi.org/10.21124/tbs.2025.306.315
ACS Style
Kooffreh-Ada,
M.; Okpokam,
D.C.; Emeng,
K.D.; Eteng,
G.T.; Ogidi,
N.O.; Opara,
C.O.; Iyamah,
E.X.; Okpokam,
O.E. Thrombin Time Clotting Assay as a Predictor Marker of Bleeding Risk in Individuals with Non-Alcoholic Fatty Liver Disease in Calabar, Nigeria. Trends Biol. Sci 2025, 1, 306-315. https://doi.org/10.21124/tbs.2025.306.315
AMA Style
Kooffreh-Ada
M, Okpokam
DC, Emeng
KD, Eteng
GT, Ogidi
NO, Opara
CO, Iyamah
EX, Okpokam
OE. Thrombin Time Clotting Assay as a Predictor Marker of Bleeding Risk in Individuals with Non-Alcoholic Fatty Liver Disease in Calabar, Nigeria. Trends in Biological Sciences. 2025; 1(4): 306-315. https://doi.org/10.21124/tbs.2025.306.315
Chicago/Turabian Style
Kooffreh-Ada, Mbang, Dorathy Chioma Okpokam, Kitu David Emeng, Gift Thomas Eteng, Nkeiruka Ogo Ogidi, Chukwuka Onyedikachim Opara, Ehijie Xavier Iyamah, and Ogha Eyamnzie Okpokam.
2025. "Thrombin Time Clotting Assay as a Predictor Marker of Bleeding Risk in Individuals with Non-Alcoholic Fatty Liver Disease in Calabar, Nigeria" Trends in Biological Sciences 1, no. 4: 306-315. https://doi.org/10.21124/tbs.2025.306.315

This work is licensed under a Creative Commons Attribution 4.0 International License.