Malaria Prevalence in Children Under Five and Pregnant Women in Hong LGA
-
A. Atinga


Department of Public Health, Taraba State College of health Technology Takum, Taraba State, Nigeria
T. GalayaDepartment of Integrated Science, Adamawa State College of Education, Hong, Nigeria
Wama Binga EmmanuelDepartment of Biological Science, Faculty of Sciences, Taraba State University, Jalingo 672101, Nigeria
O. BensonDepartment of Public Health, Taraba State College of health Technology Takum, Taraba State, Nigeria
Bolozimo Wachap ThomasDepartment of Public Health, Taraba State College of health Technology Takum, Taraba State, Nigeria
Baraya Aminu KadunaDepartment of Public Health, Taraba State College of health Technology Takum, Taraba State, Nigeria
| Received 14 Jan, 2026 |
Accepted 16 May, 2026 |
Published 30 Jun, 2026 |
Background and Objective: Malaria remains a leading cause of morbidity and mortality in Sub-Saharan Africa, disproportionately affecting pregnant women and children under five. Locally specific prevalence data are essential to guide targeted control and elimination strategies. This study aimed to determine the prevalence of malaria infection among these high-risk groups attending healthcare facilities in Hong Local Government Area, Nigeria. Materials and Methods: A cross-sectional study was conducted among 427 pregnant women and 399 children aged ≤5 years across three healthcare facilities. Malaria infection was diagnosed using rapid diagnostic tests and confirmed with Giemsa-stained blood smear microscopy. Sociodemographic and clinical data were collected, and associations with malaria infection were evaluated using Chi-square tests. Statistical significance was set at p<0.05. Results: Overall malaria prevalence was 29.5% (126/427) in pregnant women and 24.8% (99/399) in children. Among pregnant women, infection was highest in the 22-26-year age group (29.4%) and during the first trimester at the tertiary facility (40.6%), though no significant associations were observed with maternal age (χ2 = 3.21, p = 0.52) or gestational age. In children, prevalence increased with age, from 17.5% in neonates to 25.9% in toddlers (1-5 years), with no significant differences by age or gender. Facility-level comparisons revealed the highest mean malaria positivity at the tertiary hospital (27.5%), followed by Banshika (26.7%) and Hildi (25.4%). Conclusion: Malaria infection remains prevalent among pregnant women and young children in the study area, reflecting persistent gaps in preventive measures. Strengthened, facility-based interventions-including routine screening during antenatal and pediatric visits, improved access to chemoprevention, and community-targeted education-are urgently needed to reduce transmission and protect these vulnerable populations.
| Copyright © 2026 Atinga et al. This is an open-access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. |
INTRODUCTION
Malaria remains a major public health challenge in Sub-Saharan Africa, disproportionately affecting vulnerable populations such as pregnant women and children under five1. In Nigeria, malaria accounted for 17.2% of deaths and 29.1% of outpatient consultations in 2021, with children under five and pregnant women bearing a particularly high burden1,2. Hospital admissions due to malaria represented 40.1% among children under five and 22.5% among pregnant women in the same year, highlighting the ongoing impact of the disease despite population growth2.
Over the past two decades, significant progress in malaria control has been achieved globally through a combination of vector control strategies and effective treatment regimens3. Insecticide-treated nets (ITNs) and other preventive measures have contributed to substantial reductions in malaria morbidity and mortality4. However, Sub-Saharan Africa remains highly vulnerable, accounting for the majority of global malaria cases and deaths3. In 2023, malaria caused approximately 597,000 deaths worldwide, with 263 million new cases reported; Africa accounted for 94% of cases and 95% of deaths, with Nigeria alone responsible for 25% of cases and 30% of deaths5,6. Notably, 39.3% of malaria deaths in Nigeria occurred among children under five7.
In response, the Nigerian National Malaria Control Programme (NMCP), in collaboration with multiple stakeholders, has implemented a multifaceted strategy targeting malaria prevention and treatment. Key interventions include mass distribution of free ITNs during campaigns and antenatal clinic visits, seasonal malaria chemoprevention (SMC) for children aged 3-59 months in high-transmission regions, and free or subsidized treatment for malaria among children under five and the broader population6,8,9. Mass ITN campaigns launched in 2011 and reinforced in 2015 and 2019 have relied primarily on pyrethroid-treated nets. However, the effectiveness of these interventions is increasingly threatened by rising insecticide resistance in Anopheles mosquito populations, as well as challenges in sustaining high coverage and consistent use of preventive measures10,11.
Despite these control efforts, malaria continues to pose a serious health risk to pregnant women and young children, particularly in endemic regions such as Northeastern Nigeria. High prevalence rates in these groups not only increase morbidity and mortality but also contribute to adverse pregnancy outcomes, including maternal anaemia, low birth weight, and preterm delivery12,13. Similarly, malaria in children under five is associated with severe anaemia, impaired cognitive development, and elevated risk of death14,15. The persistence of malaria in these vulnerable populations underscores the urgent need for enhanced surveillance, strengthened facility-based interventions, and targeted community education to mitigate transmission and improve health outcomes.
Given this context, the present study aimed to assess malaria prevalence among pregnant women and children under five attending healthcare facilities across Hong Local Government Area, Nigeria. The findings provide critical, locally relevant data to guide more effective malaria prevention and control strategies in these high-risk groups.
MATERIALS AND METHODS
Study area: The study was conducted at Adamawa State College of Education Hong, situated in the Hong Local Government area of Adamawa State, where the local government headquarters is also located. This region falls under the Adamawa Central Senatorial District and the Gombi/Hong Federal Constituency. Geographically, Hong is positioned at approximately 100°09’44"N and 12°00’44"E.
Ethics statement: The research was performed in accordance with the ethical standards outlined in the Declaration of Helsinki and approved by the Adamawa State Ministry of Health Research Ethics Committee (ADHREC 15/10/2024/045), and written informed consent was obtained from each participant. Informed consent has also been obtained from a parent and/or legal guardian for participants below 16. The clinical trial number is not applicable in this study.
Study design: This investigation employed a cross-sectional framework, conducted across three (3) primary healthcare facilities-including General Hospital Hong, Banshika Primary Healthcare (PHC) and Hildi Clinic strategically situated within four administrative wards of Hong Local Government Area, Adamawa State. It was carried out at the peak period of malaria prevalence (September to October 2025). The facility selection ensured geographic representation to evaluate region-specific alignment with Nigeria’s public health objectives for evidence-based intervention planning in semi-urban and rural zones. The sample size for each facility was determined using the Krejcie and Morgan15 sample size formula for finite populations16. The total sample size comprised 427 pregnant women and 399 children under five across the 3-health (PHC Hildi: 108, PHC Banshika: 118, and General Hospital Hong: 201) and 399 children under five ( PHC Hildi: 127, PHCC Banshika: 113, and General Hospital Hong: 270).
Rapid diagnostic test (RDT): Malaria infection was assessed using the CareStart Malaria HRP2 Rapid Diagnostic Test, which detects Plasmodium falciparum histidine-rich protein 2 (PfHRP2), among children under five years of age. The test was performed according to the manufacturer’s instructions17,18. Briefly, 5 μL of capillary blood obtained via sterile finger prick was applied to the sample well of the test cassette, followed by the addition of assay buffer. Results were read after 15-20 minutes. The presence of both control and test lines indicated a positive result, while the presence of only the control line indicated a negative result. Tests without a visible control line were considered invalid and repeated. According to manufacturer reports and independent field evaluations, the CareStart™ PfHRP2 RDT demonstrates sensitivity greater than 95% and specificity above 90% at parasite densities ≥100 parasites/μL (Access Bio, 2015; World Health Organization [WHO], 2023). Quality control measures included storage of RDT kits at recommended temperatures (4-30°C), monitoring of expiry dates, use of desiccants to prevent moisture damage, and periodic cross-checking of 10% of RDT results with microscopy findings. All procedures were conducted in accordance with standard malaria diagnostic guidelines outlined by the World Health Organization19.
For pregnant women, capillary blood (5 μL) was also collected via sterile finger prick for confirmatory microscopy. Thick and thin blood smears were prepared on clean, grease-free slides, air-dried, and stained with 10% Giemsa solution following WHO-recommended protocols19. Microscopic examination was performed under oil immersion using a 100× objective lens (1000× total magnification). Thick smears were used to determine parasite presence and density, while thin smears were used for species identification. A malaria-positive result was defined as the detection of one or more asexual stages of Plasmodium parasites on microscopy. For quality assurance, each slide was independently examined by two experienced microscopists, and discordant results were resolved by a third reader. A minimum of 100 high-power fields was examined before declaring a slide negative19.
Data analysis procedures: Data were entered and cleaned using Microsoft Excel (Microsoft Corp., USA) and exported to IBM SPSS Statistics (IBM Corporation, USA) for statistical analysis. Descriptive statistics were computed to determine frequencies and percentages of malaria infection among pregnant women and children under five years across the three health facilities. The Chi-square (χ²) test of independence was used to examine associations between malaria infection status (positive/negative) and categorical variables, including maternal age group, gestational age (trimester), child age group, gender, and health facility. Cohen’s kappa (κ) coefficient was calculated to assess agreement between Rapid Diagnostic Test (RDT) results and microscopy findings. Statistical significance was set at p<0.05, and all tests were two-tailed.
RESULTS
Malaria infection prevalence in General Hospital Hong: A total of 201 pregnant women were examined at General Hospital Hong, of whom 69 (34.3%) tested positive for malaria. Malaria prevalence varied across age groups, with higher proportions observed among women aged 22-26 years (29.0%) and ≤21 years
| Table 1: | Malaria prevalence in pregnant women by age group (General Hospital Hong) | |||
| Variable | Total examined (%) | Positive (%) | Negative (%) | χ2 , p-value |
| ≤21 | 40 (19.9) | 18 (26.1) | 22 (16.7) | χ2 = 3.21, p = 0.52 (NS) |
| 22-26 | 55 (27.4) | 20 (29.0) | 35 (26.5) | |
| 27-31 | 50 (24.9) | 15 (21.7) | 35 (26.5) | |
| 32-36 | 35 (17.4) | 10 (14.5) | 25 (18.9) | |
| 37 above | 21 (10.4) | 6 (8.7) | 15 (11.4) | |
| Total | 201 (100.0) | 69 (34.3) | 132 (65.7) | |
| χ2: Chi-square test of independence, p: Probability value, NS: Not statistically significant. Statistical significance was set at p<0.05 | ||||
| Table 2: | Malaria prevalence in pregnant women by gestational age (General Hospital Hong) | |||
| Variable/Trimester | Total examined (%) | Positive (%) | Negative (%) | χ2 , p-value |
| First trimester | 60 (29.9) | 28 (40.6) | 32 (24.2) | χ2 = 4.12, p = 0.13 (NS) |
| Second trimester | 95 (47.3) | 30 (43.5) | 65 (49.2) | |
| Third trimester | 46 (22.9) | 11 (15.9) | 35 (26.5) | |
| Total | 201 (100.0) | 69 (34.3) | 132 (65.7) | |
| Trimester classification: First (≤13 weeks), Second (14-27 weeks), Third (≥28 weeks). χ2: Chi-square test, p: Probability value, NS: Not statistically significant. Statistical significance was set at p<0.05 | ||||
| Table 3: | Malaria infection rates by age group among children ≤5 years (General Hospital Hong) | |||
| Age group | Total examined (%) | Positive (%) | Negative (%) | χ2 , p-value |
| Neonates (1-28 days) | 15 (9.4) | 2 (6.9) | 13 (10.0) | χ2 = 1.42, p = 0.49 (NS) |
| Infants (29-12 months) | 50 (31.4) | 8 (27.6) | 42 (32.3) | |
| Toddlers (1-5 years) | 94 (59.1) | 19 (65.5) | 75 (57.7) | |
| Total | 159 (100) | 29 (18.2) | 130 (81.8) | |
| χ2: Chi-square test, p: Probability value, NS: Not statistically significant. Statistical significance was set at p<0.05 | ||||
| Table 4: | Prevalence of malaria infection by gender among children ≤5 years (General Hospital Hong) | |||
| Gender | Total examined (%) | Positive (%) | Negative (%) | χ2, p-value |
| Male | 84 (52.8) | 15 (51.7) | 69 (52.7) | χ2 = 0.03, p = 0.86 (NS) |
| Female | 75 (47.2) | 14 (48.3) | 61 (47.3) | |
| Total | 159 (100) | 29 (18.2) | 130 (81.8) | |
| χ2 = Chi-square test, p: Probability value, NS: Not statistically significant. Statistical significance was set at p<0.05 | ||||
(26.1%), and lower prevalence among women aged ≥37 years (8.7%). However, maternal age was not significantly associated with malaria infection (χ2 = 3.21, p = 0.52), Table 1. By gestational age, malaria prevalence was highest in the first trimester (40.6%) and lowest in the third trimester (15.9%), with no statistically significant association detected (χ2 = 4.12, p = 0.13), as shown in Table 2.
Among 159 children aged ≤5 years in Table 3, 29 (18.2%) tested positive for malaria. Infection prevalence increased with age, from 13.3% in neonates to 20.2% among toddlers aged 1-5 years, though this trend was not statistically significant (χ2 = 1.42, p = 0.49). Malaria prevalence was comparable between males (17.9%) and females (18.7%), with no significant gender difference (χ2 = 0.03, p = 0.86), Table 4.
Malaria infection prevalence in Banshika Primary Health Care (PHC): About 108 pregnant women were assessed, with 28 (25.9%) testing positive for malaria. Higher prevalence was observed among women aged ≤21 years (31.8%) and 22-26 years (30.0%), while lower prevalence occurred among women aged ≥32 years. Maternal age showed no significant association with malaria infection (χ2 ≈ 1.26, p ≈ 0.87), as shown in Table 5. Malaria prevalence by gestational age ranged from 22.7% to 31.3%, with no statistically significant difference across trimesters (χ2 ≈ 0.72, p ≈ 0.70) Table 6.
Among 113 children aged ≤5 years, 34 (30.1%) were malaria-positive. Prevalence was highest among infants (35.0%), followed by toddlers aged 1-5 years (28.6%) and neonates (20.0%), with no significant association between age group and malaria infection (χ2 = 1.01, p = 0.60) Table 7. Malaria prevalence did not differ significantly between males (33.3%) and females (26.4%) (χ2 = 0.35, p = 0.55) Table 8.
| Table 5: | Malaria prevalence in pregnant women by age group (Banshika) | |||
| Variable | Total examined (%) | Positive (%) | Negative (%) | χ2 , pvalue |
| ≤21 | 22 (20.4) | 7 (31.8) | 15 (68.2) | χ2 ≈ 1.26, df = 4, p ≈ 0.867 |
| 22-26 | 30 (27.8) | 9 (30.0) | 21 (70.0) | |
| 27-31 | 27 (25.0) | 6 (22.2) | 21 (77.8) | |
| 32-36 | 19 (17.6) | 4 (21.1) | 15 (78.9) | |
| 37 above | 10 (9.3) | 2 (20.0) | 8 (80.0) | |
| Total | 108 (100) | 28 (25.9) | 80 (74.1) | |
| χ2: Chi-square test, p: Probability value, df: Degrees of freedom, NS: Not statistically significant. Statistical significance was set at p<0.05 | ||||
| Table 6: | Malaria prevalence in pregnant women by gestational age (Banshika) | |||
| Variable/Trimester | Total examined (%) | Positive (%) | Negative (%) | χ2 , pvalue |
| First trimester | 32 (29.6) | 10 (31.3) | 22 (68.7) | χ2 ≈ 0.72, df = 2, p ≈ 0.696 |
| Second trimester | 44 (40.7) | 10 (22.7) | 34 (77.3) | |
| Third trimester | 32 (29.6) | 8 (25.0) | 24 (75.0) | |
| Total | 108 (100) | 28 (25.9) | 80 (74.1) | |
| Trimester classification: First (≤13 weeks), Second (14-27 weeks), Third (≥28 weeks). χ2: Chi-square test, p: Probability value, df: Degrees of freedom, NS: Not statistically significant. Statistical significance was set at p<0.05 | ||||
| Table 7: | Malaria infection rates by age group among children ≤5 years (Banshika) | |||
| Age groups | Total examined (%) | Positive (%) | Negative (%) | χ2, pvalue |
| Neonates (1-28 days) | 10 (8.8) | 2 (20.0) | 8 (80.0) | χ2 = 1.01, p = 0.60 (NS) |
| Infants (29-12 months) | 40 (35.4) | 14 (35.0) | 26 (65.0) | |
| Toddler 1-5 years old | 63 (55.8) | 18 (28.6) | 45 (71.4) | |
| Total | 113 (100) | 34 (30.1) | 79 (69.9) | |
| χ2: Chi-square test, p: Probability value, NS: Not statistically significant. Statistical significance was set at p<0.05 | ||||
| Table 8: | Prevalence of malaria infection by gender among children ≤5 years (Banshika) | |||
| Age groups | Total examined (%) | Positive (%) | Negative (%) | χ2 , p-value |
| Male | 60 (53.1) | 20 (33.3) | 40 (66.7) | χ2 = 0.35, p = 0.55 (NS) |
| Female | 53 (46.9) | 14 (26.4) | 39 (73.6) | |
| Total | 113 (100) | 34 (30.1) | 79 (69.9) | |
| χ2: Chi-square test, p: Probability value, NS: Not statistically significant. Statistical significance was set at p<0.05 | ||||
| Table 9: | Malaria prevalence in pregnant women by age group (Hildi Clinic) | |||
| Age group | Total examined (%) | Positive (%) | Negative (%) | χ2, p-value |
| ≤21 | 22 (18.6) | 7 (24.1) | 15 (16.9) | χ2 = 0.95, p = 0.92 (NS) |
| 22-26 | 33 (28.0) | 8 (27.6) | 25 (28.1) | |
| 27-31 | 30 (25.4) | 6 (20.7) | 24 (27.0) | |
| 32-36 | 20 (16.9) | 5 (17.2) | 15 (16.9) | |
| 37 above | 13 (11.0) | 3 (10.3) | 10 (11.2) | |
| Total | 118 (100) | 29 (24.6) | 89 (75.4) | |
| χ2: Chi-square test, p: Probability value, NS: Not statistically significant. Statistical significance was set at p<0.05 | ||||
| Table 10: | Malaria prevalence in pregnant women by gestational age (Hildi Clinic) | |||
| Trimester | Total examined (%) | Positive (%) | Negative (%) | χ2, p-value |
| First trimester | 40 (33.9) | 12 (41.4) | 28 (31.5) | χ2 = 1.82, p = 0.40 (NS) |
| Second trimester | 50 (42.4) | 12 (41.4) | 38 (42.7) | |
| Third trimester | 28 (23.7) | 5 (17.2) | 23 (25.8) | |
| Total | 118 (100) | 29 (24.6) | 89 (75.4) | |
| χ2: Chi-square test, p: Probability value, NS: Not statistically significant. Statistical significance was set at p<0.05 | ||||
Malaria infection prevalence in Hildi Primary Health Care (PHC): A 118 pregnant women were examined, of whom 29 (24.6%) tested positive for malaria. Malaria prevalence was highest among women aged ≤26 years, with decreasing prevalence in older age groups; however, the association between age and malaria infection was not statistically significant (χ2 = 0.95, p = 0.92) Table 9. By gestational age, malaria prevalence was higher in the first and second trimesters (41.4% each) compared with the third trimester (17.2%), though no significant association was observed (χ2 = 1.82, p = 0.40), Table 10.
|
| Table 11: | Malaria infection rates by age group among children ≤5 years (Hildi Clinic) | |||
| Variable (Age group) | Total examined (%) | Positive (%) | Negative (%) | χ2, p-value |
| Neonates (1-28 days) | 15 (11.8) | 3 (8.3) | 12 (13.2) | χ2 = 1.12, p = 0.57 (NS) |
| Infants (29-12 months) | 45 (35.4) | 12 (33.3) | 33 (36.3) | |
| Toddlers (1-5 years) | 67 (52.8) | 21 (58.4) | 46 (50.5) | |
| Total | 127 (100.0) | 36 (28.3) | 91 (71.7) | |
| χ2: Chi-square test, p: Probability value, NS: Not statistically significant. Statistical significance was set at p<0.05 | ||||
| Table 12: | Prevalence of malaria infection by gender among children ≤5 years (Hildi Clinic) | |||
| Gender | Total examined (%) | Positive (%) | Negative (%) | χ2, p-value |
| Male | 66 (51.9) | 19 (52.8) | 47 (51.6) | χ2 = 0.01, p = 0.92 (NS) |
| Female | 61 (48.1) | 17 (47.2) | 44 (48.4) | |
| Total | 127 (100) | 36 (28.3) | 91 (71.7) | |
| χ2: Chi-square test, p: Probability value, NS: Not statistically significant. Statistical significance was set at p<0.05 | ||||
| Table 13: | Overall malaria prevalence in pregnant women by age group | |||
| Age group | Total examined (%) | Positive (%) | Negative (%) | χ2, p-value |
| ≤21 | 84 (19.7) | 32 (25.4) | 52 (17.2) | χ2= 3.21, p = 0.52 (NS) |
| 22-26 | 118 (27.6) | 37 (29.4) | 81 (26.8) | |
| 27-31 | 107 (25.1) | 27 (21.4) | 80 (26.5) | |
| 32-36 | 74 (17.3) | 19 (15.1) | 55 (18.2) | |
| 37 above | 44 (10.3) | 11 (8.7) | 33 (10.9) | |
| Total | 427 (100.0) | 126 (29.5) | 301 (70.5) | |
| χ2: Chi-square test, p: Probability value, NS: Not statistically significant. Statistical significance was set at p<0.05 | ||||
| Table 14: | Overall malaria infection rates by age group among children ≤5 years | |||
| Age group | Total examined (%) | Positive (%) | Negative (%) | χ2, p-value |
| Neonates (1-28 days) | 40 (10.0) | 7 (17.5) | 33 (82.5) | χ2 = 1.42, p = 0.49 (NS) |
| Infants (29 days-12 months) | 135 (33.8) | 34 (25.2) | 101 (74.8) | |
| Toddlers (1-5 years) | 224 (56.1) | 58 (25.9) | 166 (74.1) | |
| Total | 399 (100.0) | 99 (24.8) | 300 (75.2) | |
| χ2: Chi-square test, p: Probability value, NS: Not statistically significant. Statistical significance was set at p<0.05 | ||||
Among 127 children aged ≤5 years, 36 (28.3%) tested positive for malaria. Prevalence increased with age, from 20.0% in neonates to 31.3% among toddlers aged 1-5 years, but this difference was not statistically significant (χ2 = 1.12, p = 0.57), Table 11. Malaria prevalence was similar between males (28.8%) and females (27.9%) (χ2 = 0.01, p = 0.92) Table 12.
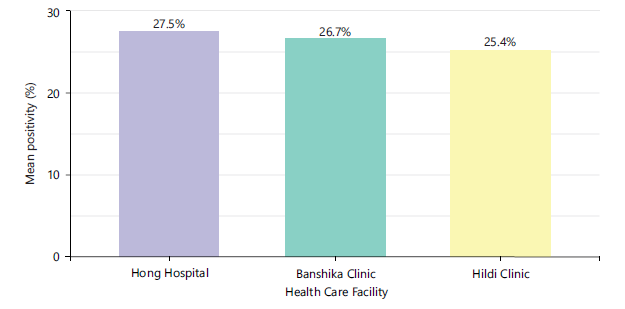
Overall malaria prevalence: Overall malaria prevalence across the three facilities is shown in Fig. 1, with Hong Hospital (27.5%) having the highest mean positivity, followed by Banshika (26.7%) and Hildi (25.4%). Across all sites, 427 pregnant women were examined, with 126 (29.5%) testing positive; prevalence was
highest among women aged 22-26 years (29.4%) and lowest in those aged ≥37 years (8.7%), with no significant association by age (χ2 = 3.21, p = 0.52) Table 13. Among 399 children ≤5 years, 99 (24.8%) were malaria-positive, increasing from 17.5% in neonates to 25.9% in toddlers, with age group not significantly associated with infection (χ2 = 1.42, p = 0.49) Table 14.
DISCUSSION
This study provides a critical snapshot of the malaria burden among two highly vulnerable populations-pregnant women and children under five-attending three healthcare facilities in a malaria-endemic region. The key findings reveal a persistently high prevalence of malaria infection, with nearly one-third of pregnant women (29.5%) and one-quarter of children under five (24.8%) testing positive. Notably, while certain demographic and clinical trends were observed-such as higher prevalence in younger pregnant women and during early pregnancy-no statistically significant associations were found for age, gestational trimester, or child's gender at any individual site or in the pooled analysis. These results underscore the pervasive nature of malaria transmission in the region and highlight the urgent need for reinforced, site-tailored intervention strategies that go beyond demographic targeting.
The overall malaria prevalence of 29.5% among pregnant women is alarmingly high and considerably exceeds figures reported in several recent Sub-Saharan African studies, where prevalence in antenatal cohorts often ranges from 10-20%19,20. This elevated burden signals potential gaps in the coverage or effectiveness of standard preventive measures, such as Intermittent Preventive Treatment in pregnancy (IPTp) and insecticide-treated net (ITN) distribution. The trend of higher infection rates among younger women (≤26 years), though not statistically significant, is clinically concerning and echoes established literature indicating that primigravidae and younger women possess lower acquired immunity to Plasmodium falciparum21. The observed gradient, with the lowest prevalence in women aged ≥37 years, further supports the role of acquired immunity developed over successive pregnancies and exposures.
Similarly, the pattern of highest prevalence in the first trimester (40.6% at Hong Hospital) aligns with the physiological nadir of immunity during early pregnancy22. The subsequent decline across trimesters may reflect the initiation or increased uptake of antenatal care (ANC) and IPTp later in pregnancy. However, the non-significant p-value (p = 0.13) for this association at Hong Hospital, and across all sites, suggests substantial inter-individual variation and potentially confounding factors like ITN use, parity, and proximity to vector breeding sites. The lack of statistical significance should not be misinterpreted as a lack of public health importance; rather, it may reflect the limited sample size within trimester subgroups, which reduces statistical power to detect true differences.
Among children under five, the prevalence of 24.8% represents a substantial disease burden contributing to childhood morbidity, including anaemia and impaired cognitive development23. The consistent trend of increasing prevalence from neonates to toddlers across all facilities is expected, as neonates benefit from passive maternal immunity and reduced exposure, while toddlers have greater environmental exposure and waning maternal protection24,25. Again, the non-significant association likely points to sample size limitations in the neonatal subgroup. The absence of any gender difference in infection rates is consistent with the biological expectation that susceptibility to malaria in early childhood is not sex-specific, affirming that prevention programs must be universally applied to all children in this age bracket.
The comparative analysis between facilities reveals important nuances. General Hospital Hong reported the highest prevalence in both pregnant women (34.3%) and children (18.2%), which may be attributed to its status as a referral centre attracting more severe or complicated cases from a wider catchment area. In contrast, the two PHCs (Banshika and Hildi) showed slightly lower but still substantial prevalence, possibly reflecting more localized transmission dynamics or varied levels of community engagement with primary health services. These differences highlight that while malaria is a ubiquitous threat, hyper-local epidemiological factors necessitate facility-specific and community-specific strengthening of control measures.
DATA ACCESSIBILITY
The datasets generated and analyzed during this research are publicly available as an attachment in the supplementary file.
ETHICAL COMPLIANCE
Documented informed consent was acquired from all individuals involved in this study, including co-authors and participants, before the publication of research findings. This process aligned with institutional ethical standards and review board requirements.
DECLARATION OF INTERESTS
The authors confirm no financial, professional, or personal conflicts of interest that could be perceived as influencing the impartiality, methodology, or conclusions presented in this work.
CONCLUSION
This study demonstrates a persistently high burden of malaria among pregnant women (29.5%) and children under five (24.8%) in three healthcare facilities within a malaria-endemic region. Although no statistically significant associations were observed with maternal age, gestational trimester, child age, or gender, trends indicate higher infection rates among younger women, early pregnancy, and toddlers. The findings highlight gaps in current preventive strategies, including IPTp and ITN coverage, and emphasize the need for targeted, context-specific interventions. Strengthening facility- and community-level malaria control measures, with universal coverage for high-risk populations, is critical to reducing transmission and improving maternal and child health outcomes in the region.
SIGNIFICANCE STATEMENT
This study provides locally specific data on malaria prevalence among pregnant women and children under five in Hong Local Government Area, Nigeria, highlighting persistent transmission despite existing control measures. The findings emphasize the urgent need for strengthened facility-based interventions, routine screening, and community-targeted education to protect vulnerable populations and guide evidence-based malaria prevention and elimination strategies in high-risk regions.
REFERENCES
- Okello, G. and M. Aucamp, 2026. Malaria: A review on its current epidemiological status and management strategies. Malar. J., 25.
- Kamau, A., P. Mogeni, E.A. Okiro, R.W. Snow and P. Bejon, 2020. A systematic review of changing malaria disease burden in Sub-Saharan Africa since 2000: Comparing model predictions and empirical observations. BMC Med., 18.
- Merga, H., T. Degefa, Z. Birhanu, A. Tadele, M.C. Lee, G. Yan and D. Yewhalaw, 2025. Urban malaria in Sub-Saharan Africa: A scoping review of epidemiologic studies. Malar. J., 24.
- Bhatt, S., D.J. Weiss, E. Cameron, D. Bisanzio and B. Mappin et al., 2015. The effect of malaria control on Plasmodium falciparum in Africa between 2000 and 2015. Nature, 526: 207-211.
- Noor, A.M., D.K. Kinyoki, C.W. Mundia, C.W. Kabaria and J.W. Mutua et al., 2014. The changing risk of Plasmodium falciparum malaria infection in Africa: 2000-10: A spatial and temporal analysis of transmission intensity. Lancet, 383: 1739-1747.
- WHO, 2021. World Malaria Report 2021. World Health Organization, Geneva, Switzerland, ISBN: 9789240040496, Pages: 263.
- Hancock, P.A., C.J.M. Hendriks, J.A. Tangena, H. Gibson and J. Hemingway et al., 2020. Mapping trends in insecticide resistance phenotypes in African malaria vectors. PLoS Biol., 18.
- Sinka, M.E., M.J. Bangs, S. Manguin, Y. Rubio-Palis and T. Chareonviriyaphap et al., 2012. A global map of dominant malaria vectors. Parasites Vectors, 5.
- Tusting, L.S., C. Bottomley, H. Gibson, I. Kleinschmidt, A.J. Tatem, S.W. Lindsay and P.W. Gething, 2017. Housing improvements and malaria risk in Sub-Saharan Africa: A multi-country analysis of survey data. PLoS Med., 14.
- Msugupakulya, B.J., N.H. Urio, M. Jumanne, H.S. Ngowo, P. Selvaraj, F.O. Okumu and A.L. Wilson, 2023. Changes in contributions of different Anopheles vector species to malaria transmission in East and Southern Africa from 2000 to 2022. Parasites Vectors, 16.
- Killeen, G.F., 2014. Characterizing, controlling and eliminating residual malaria transmission. Malar. J., 13.
- Gillies, M.T. and B. de Meillon, 1968. The Anophelinae of Africa South of the Sahara (Ethiopian Zoogeographical Region). 2nd Edn., South Africa Institute for Medical Research, Johannesburg, South Africa, Pages: 343.
- Gillies, M.T. and M. Coetzee, 1987. A Supplement to the Anophelinae of Africa South of the Sahara (Afrotropical Region). South African Institute for Medical Research, Johannesburg, ISBN-13: 9780620103213, Pages: 143.
- Scott, J.A., W.G. Brogdon and F.H. Collins, 1993. Identification of single specimens of the Anopheles gambiae complex by the polymerase chain reaction. Am. J. Trop. Med. Hygiene, 49: 520-529.
- Krejcie, R.V. and D.W. Morgan, 1970. Determining sample size for research activities. Educ. Psychol. Meas., 30: 607-610.
- Symons, T.L., A. Moran, A. Balzarolo, C. Vargas and M. Robertson et al., 2026. Projected impacts of climate change on malaria in Africa. Nature, 651: 390-396.
- White, N.J., S. Pukrittayakamee, T.T. Hien, M.A. Faiz, O.A. Mokuolu and A.M. Dondorp, 2014. Malaria. Lancet, 383: 723-735.
- Oyegoke, O.O., L. Maharaj, O.P. Akoniyon, I. Kwoji and A.T. Roux et al., 2022. Malaria diagnostic methods with the elimination goal in view. Parasitol Res., 121: 1867-1885.
- Desai, M., F.O. ter Kuile, F. Nosten, R. McGready, K. Asamoa, B. Brabin and R.D. Newman, 2007. Epidemiology and burden of malaria in pregnancy. Lancet Infect. Dis., 7: 93-104.
- van Eijk, A.M., J. Hill, A.M. Noor, R.W. Snow and F.O. ter Kuile, 2015. Prevalence of malaria infection in pregnant women compared with children for tracking malaria transmission in Sub-Saharan Africa: A systematic review and meta-analysis. Lancet Global Health, 3: e617-e628.
- Kotepui, M., K.U. Kotepui, F.R. Masangkay, A. Mahittikorn and P. Wilairatana, 2023. Prevalence and proportion estimate of asymptomatic Plasmodium infection in Asia: A systematic review and meta-analysis. Sci. Rep., 13.
- Rogerson, S.J., L. Hviid, P.E. Duffy, R.F.G. Leke and D.W. Taylor, 2007. Malaria in pregnancy: Pathogenesis and immunity. Lancet Infect. Dis., 7: 105-117.
- Nankabirwa, J., S.J. Brooker, S.E. Clarke, D. Fernando, C.W. Gitonga, D. Schellenberg and B. Greenwood, 2014. Malaria in school-age children in Africa: An increasingly important challenge. Trop. Med. Int. Health, 19: 1294-1309.
- Ding, X.C., S. Incardona, E. Serra-Casas, S.C. Charnaud and H.C. Slater et al., 2023. Malaria in pregnancy (MiP) studies assessing the clinical performance of highly sensitive rapid diagnostic tests (HS-RDT) for Plasmodium falciparum detection. Malar. J., 22.
- Kattenberg, J.H., E.A. Ochodo, K.R. Boer, H.D.F.H. Schallig, P.F. Mens and M.M.G. Leeflang, 2011. Systematic review and meta-analysis: Rapid diagnostic tests versus placental histology, microscopy and PCR for malaria in pregnant women. Malar. J., 10.
How to Cite this paper?
APA-7 Style
Atinga,
A., Galaya,
T., Emmanuel,
W.B., Benson,
O., Thomas,
B.W., Kaduna,
B.A. (2026). Malaria Prevalence in Children Under Five and Pregnant Women in Hong LGA. Trends in Biological Sciences, 2(2), 219-227. https://doi.org/10.21124/tbs.2026.219.227
ACS Style
Atinga,
A.; Galaya,
T.; Emmanuel,
W.B.; Benson,
O.; Thomas,
B.W.; Kaduna,
B.A. Malaria Prevalence in Children Under Five and Pregnant Women in Hong LGA. Trends Biol. Sci 2026, 2, 219-227. https://doi.org/10.21124/tbs.2026.219.227
AMA Style
Atinga
A, Galaya
T, Emmanuel
WB, Benson
O, Thomas
BW, Kaduna
BA. Malaria Prevalence in Children Under Five and Pregnant Women in Hong LGA. Trends in Biological Sciences. 2026; 2(2): 219-227. https://doi.org/10.21124/tbs.2026.219.227
Chicago/Turabian Style
Atinga, A., T. Galaya, Wama Binga Emmanuel, O. Benson, Bolozimo Wachap Thomas, and Baraya Aminu Kaduna.
2026. "Malaria Prevalence in Children Under Five and Pregnant Women in Hong LGA" Trends in Biological Sciences 2, no. 2: 219-227. https://doi.org/10.21124/tbs.2026.219.227

This work is licensed under a Creative Commons Attribution 4.0 International License.